| Poisoning For Profits | Source |
 |
Poisoning for Profit goes on a deep dive investigating the very origin of the vitamin A theory. The author uncovers that the early scientific studies conducted in the 1920s used to establish so-called vitamin A being a “vitamin” were grossly flawed and therefore almost meaningless. Ironically, what these early studies did establish was the incredible, yet previously unknown and hidden, toxicity of so-called vitamin A. The author goes deeper and proposes that vitamin A is not actually a vitamin at all; rather it is a toxin, and only a toxin. However, vitamin A is a toxin that the human body is well prepared to deal with, but it can only handle it at a reasonable rate of consumption.
Tragically, based on the botched science from the 1920s the world has been led into a massive health disaster by having many of our common staple foods supplemented with an insidious toxin. The author explains and details the mechanism of how this so-called vitamin is likely responsible for many of the modern-day chronic diseases plaguing humanity. The primary diseases implicated are the autoimmune diseases, many soft-tissue cancers, IBD and other inflammatory diseases, infertility and the psychiatric diseases of epilepsy, schizophrenia, Alzhiemer’s / dementia.
Poisoning for Profit ends with a call to action for a grassroots and worldwide citizen driven research project to determine the truth about so-called vitamin A.
| Chapter 1 Chapter 2 Chapter 3 Chapter 4 Chapter 5 Chapter 6 Chapter 7 Chapter 8 Chapter 9 Chapter 10 Chapter 11 Chapter 12 Chapter 13 Chapter 14 |
Vitamin-A theory – the early years The Experiment – the cornerstone of Science The incredible toxicity of vitamin-A The epithelial tissues - the foundation of the chronic diseases The botched deficiency experiments Real-world testing of the vitamin-A deficiency theory Vitamin-A supplementation in SE Asia, and South America Vitamin-A supplementation and Worldwide Infertility Rates Vision as a chemical reaction The greatest understanding in medicine - ever Lutein / zeaxanthin - the hidden death trap Vaccines and Vitamin-A – the perfect storm Systemic scientific fraud A Call to Action - We experiment Appendix |
1 7 9 19 33 48 54 63 66 71 76 77 96 105 121 |
 |
I am an engineer and geologist. I am 60 years old and live in Western Canada.
I have absolutely no medical experience. I am not offering or suggesting medical advice. I am not selling or promoting any product or services. My goal is to get a clear understanding of the root cause(s) of the autoimmune diseases.
If you have any questions or feedback, then please do not hesitate to contact me. The more people we have discussing this topic the faster it will get solved. Thank you.
Grant Genereux, P. Eng.
Poisoning for Profits
Edition 1.3.3, July 2017
Author Contact:
The statements herein are not intended to diagnose, treat, cure or prevent disease. The information provided is for educational purposes only and is not meant to substitute for the advice provided by your doctor or other health care professional.
There are many references in this book to external sources, most with a URL link. At the time of writing, all links were valid. However, this is the internet, and things can and do change frequently. Therefore, if you find a broken link, just search for the source document by name.
I have two goals in publishing this e-book. The first is to challenge the determination of vitamin-A as being a vitamin. The second goal is to get to the true understanding of the root-cause of the autoimmune diseases.
This book is not about opinion or endless debates; it is about the facts. It is not intended to entertain you; it is to inform you and hopefully to call you into action. This e-book is also not about making money. You may freely share this e-book under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This book is a follow-on from my previous e-book publication, titled: Extinguishing the Fires of Hell. You can download it from a link contained on the page here: https://ggenereuxblog.wordpress.com/2016/04/22/ending-the-mystery-of-auto-immune/
In that earlier work, I built up what I thought was a pretty strong case for my theory that the autoimmune diseases, and some of the other major chronic diseases of our time, are indeed rooted in subclinical vitamin-A poisoning. I presented hundreds of different pieces of information and evidence to make that case. Every single bit of that evidence was backed up by references, and much of it was published in reputable peer-reviewed scientific studies. Although no single piece of evidence presented therein was conclusive, I felt that when it was all combined, that collectively it should have been very compelling. I was trying to piece together all the smaller and seemingly disparate pieces of evidence into a mosaic that would reveal the bigger picture. I felt that in doing that, the case implicating vitamin-A in the chronic diseases would be just so logical, and so overwhelmingly clear, that most people would see it.
However, for the most part, that was not the reaction I received. From the very few people who I could even get to read that e-book, the reaction was far less than supportive. A few other people were sitting on the fence about it, and gave it a qualified maybe. Even though there were a few people who did indeed “get it,” for most folks, it was a non-starter. They were just not even considering it to be a possibility. I could have blamed this reaction on say, they were just not open minded enough, or that they just did not try hard enough to see the connections, and / or that they were not curious enough to dig into the backup research and studies, etc. But, the reality is that if anyone’s to blame, it’s me. I think I fell into the trap of thinking that more, and more, and more evidence would make the case. The truth is that I probably presented too much information, and most people just don’t have the time to read, in depth, a 400-page book on some outsider’s wacko theory. Unless people have a horse in the race, so to speak, they are just not going to make the needed time investment, and do the investigative thinking, needed to “get it.” But, that’s only part of the reason they weren’t getting it. More importantly, I believe they were just not willing to consider such a theory, regardless of the evidence. This theory was both too simplistic, and too far in left field. To paraphrase a few people, the reaction I got was: “Oh, no way, the autoimmune diseases are just far more complicated, and it can’t be explained by such a simple theory.” Therefore, all the circumstantial evidence and logical arguments I presented just weren’t cutting it. Additionally, who was I to make such absurd assertions? I was not an expert at all, and I had no background whatsoever in the field of medical science. It was like, “nope, no way, this is a job for the experts,” and you are not one of them.
People needed some big official scientific study to directly make the case for them. I dislike making this statement, but, I felt they just weren’t willing to think this through for themselves. Rather, they were deferring the thinking to the so-called experts, and medical science. Sadly, I could see that for a few of these folks, logical thinking had been replaced by procedure, and following the “official” rules and processes. However, what they may have missed is that I wanted to follow the official process of science. I wanted them to help conduct a bigger experiment. I knew and clearly stated that my theory was just that, a theory. In science, a theory remains to be a theory until other people prove it to be true. Moreover, before a theory becomes accepted, it needs to be proven true by many others, and at least hundreds, if not thousands of times over too. Therefore, my intent in writing that first e-book was to at least make the case compelling enough to have people experiment with this theory on themselves. To me, it seemed to be at least a reasonable thing to consider, since it was just a diet-change experiment. After all, the alternatives are not looking too promising since there’s been no great progress made by official medical science in getting to the root causes of these diseases. But, not too surprisingly, there have only been a few people so far who have been willing to take on this experiment. I guess you’d have to be rather open-minded, and even a bit bold to make such a dramatic sounding diet change. Of course, the big concern for everyone is the risk of vitamin-A deficiency. Surely, the official processes of medical science didn’t get that wrong? After all, for over one hundred years now, official medical science has been telling us that we’ll all quickly go blind if we don’t get enough vitamin-A each and every day. We are also told that there are millions of kids in Southeast Asia sick or even dying every year from vitamin-A deficiency. So, in the face of these little facts, it probably seems somewhat risky to go on a zero vitamin-A diet. Therefore, the question most people probably ask themselves is something like this:
I am already suffering from autoimmune disease, am I really going to take on this silly experiment, with a very long shot chance of it doing any good, and risk the very real and dire consequences of vitamin-A deficiency? Am I willing to risk going blind too?
Naturally, that is exactly the question I had seriously asked myself too. Maybe oddly, the answer was easy for me. I thought that if I had a choice between going blind or having to deal with my skin burning off due to eczema for the rest of my days, I’d take the blindness. It was a decision I made in a heartbeat. Yep, I’d rather go blind than to live in continuous pain. However, I also knew that it was not necessarily an or condition. I could end up with both blindness and continued, unabated, eczema. However, based on my preliminary four hours of research, I was rather damn sure I was not going to go blind. I had determined I had a least a year’s supply of vitamin-A stored in my liver. I was also quite sure that eczema was none other than vitamin-A poisoning.
Therefore, I thought that I’d be able to at least improve my eczema condition well before any adverse symptoms showed up in my vision. I am a numbers type guy; I trust numbers. I am also a “science” type guy. I love and understand science. I also knew that science could and does occasionally get it wrong. That is just an absolute fact. I also knew that when science does get it wrong, it was the people who were interpreting the science who got it wrong. We all make mistakes. Therefore, it was only a bit surprising to me when my vision quickly became dramatically better on my vitamin-A elimination diet.
So now, after being on a vitamin-A-free diet for over three years by avoiding retinol and carotenoids (nearly zero molecules of any of these compounds), I no longer have eczema. Also, I am not typing this on a brail keyboard! Therefore, I know that the people in medical science did indeed absolutely get it wrong here.
Unlike numbers, I don’t trust people so easily, and especially so when there are large amounts of money in the equations. Human nature is almost as predictable as math and science in this regard; when there are large amounts of money to be made, there is usually large amounts of corruption too.
Therefore, the intent of this e-book is two-fold. One is to assure you that no, you are not going to go blind on a vitamin-A deplete diet. And two, to attempt to debunk the entire vitamin-A deficiency theory. Once you have that information, I hope you will apply it to your autoimmune disease.
If you’ve skipped the preface, and haven’t read my prior e-book then you will be missing some important context of what this book is all about. Please go back and read the preface before continuing here.
My early investigation into vitamin-A has been full of surprises. It was surprising to find that there are over fifty documented symptoms of vitamin-A toxicity, and there are over fifty named autoimmune diseases. That’s correct. Almost every significant symptom of vitamin-A toxicity has a correspondingly named autoimmune disease. Yet, there were a few paradoxes too. But, the one that I found most troubling and perplexing is that the symptoms of vitamin-A toxicity. That seemed so peculiar to me. It would be somewhat like seeing that the documented symptoms of dying from dehydration as being identical to those of dying from drowning. It was just so illogical. Something was just not adding up here with vitamin-A being both a deadly toxin and a critical vitamin at the same time, and with the same symptoms if you get too much, or too little of it. Someone, somewhere just had to have gotten their wires crossed on this one. Another perplexing question I struggled with was why had the human body built such a critical dependency upon a toxic molecule. This dependency was most certainly not impossible, it just seemed strange to me that after millions of years of being perfected by evolution (or by God’s creation if you prefer), that we’d have such a dicey dependency upon this one highly toxic molecule. It was hard to believe that nature (or God) could be this foolish.
Other areas of my investigation revealed many more apparent paradoxes and completely conflicting pieces of information. Additionally, in the various studies regarding vitamin-A, almost all the contradictions and paradoxes, are conveniently explained away, or glossed over, and done so with completely unsubstantiated rationalizations. Many of the so-called medical experts who blame illness on a vitamin A deficiency are either just making it up, blindly restating unsupportable prior theories as being fact, or just down right fabricating and obfuscating study results to fit a pre-established narrative. Sadly, it goes way beyond that. I could have never imagined that medical science was so rife with blatant scientific fraud.
Moreover, after carefully reading the very detailed descriptions by leading ophthalmologists of the progression of tissue destruction in the eye due to xerophthalmia (chronic dry eyes), it was an exact match for the description and progression of the tissue destruction I witnessed under a microscope with my own skin due to eczema. It was not just an approximate match, or a very close match, it was an absolutely perfect match. Yes, I knew all about those little cone shaped piercing blisters. The only difference is the named organ where the tissue destruction was taking place. However, somehow, more than one hundred years of modern medicine has failed to see the obvious; they are indeed one and the same condition. It is exactly, and precisely, the same condition occurring in two different organs. It was immediately clear to me that xerophthalmia and eczema are the same condition occurring in both the epithelial tissues of the eye and the epidermis.
Of course, the leading theory in ophthalmology (and that promoted by the World Health Organization) is that xerophthalmia is the direct result of vitamin-A deficiency. Although I am making an extrapolation here, xerophthalmia is effectively eczema of the eye. Thus, with the de-facto causation theory of xerophthalmia being that of vitamin-A deficiency, we should be able to conversely apply the same causation theory to eczema. Meaning, the leading theory in the causation of eczema should also be vitamin-A deficiency too. Therefore, just one of the great contradictions I want to highlight here is that there are now 30 million people in North America with eczema (with various degrees of severity), and there is simply no way they are vitamin-A deficient. There is simply no way even the tiniest fraction of them are vitamin-A deficient. So, how in the hell is it that vitamin-A deficiency can cause xerophthalmia in the eye due to vitamin-A deficiency, and for us to have exactly the same condition in the skin to occur in 30 million people who are clearly not vitamin-A deficient? However, once you factor into the equation that the tissue of the skin and the eye are both this beautifully structured stratified epithelial tissue, and the very well proven destruction too much vitamin-A will induce in this particular tissue structure, the mystery and contradictions disappear. What you are about to learn, is that the truth is that xerophthalmia is not caused by vitamin-A deficiency at all. Rather it is the exact opposite; vitamin-A toxicity causes it.
Of course, I’m only scratching the surface here regarding the obvious inconsistencies and contradictions in the vitamin-A story. The other primary, and obvious, contradiction, somehow also still being glossed over by modern medical science, is that if we are all so at risk of vitamin-A deficiency, and its horrible, if not deadly, consequences of going blind, how is it that we are here as a species at all? It is so gigantically illogical, this, by itself, should have quickly thrown the vitamin-A deficiency theory into the scientific trash can of nonsense. For example, some of the early experiments putting animals (dogs, rabbits, chickens, and most often rats) on vitamin-A deficient diets, and for them to quickly develop the systemic and catastrophic destruction of all their epithelial tissues should have raised serious questions as to the validity of the design of their experiments. In dogs, the epithelial destruction happened as quickly as in four weeks; in rats, it was around eight to ten weeks. Naturally, most of the animals died shortly after that. Therefore, how is that even possible for animals to be this critically susceptible to vitamin-A deficiency, and still be on the planet as a species? Having such a disastrously inherent design flaw resulting in the eyes, and many other organs, to quickly start self-destructing and to ultimately fail due to a vitamin-A deficiency in just eight weeks would immediately rule these animals, and us too for that matter, out of evolutionary existence. Having the eyes failing in just four to eight weeks, due to vitamin-A deficiency, would obviously be an end-of-life event. Without vision, any animal would quickly be eaten by predators, and if that did not kill them, they would not be able to find their own food. In other words, if this design flaw did exist in any species, then that species would have long ago become extinct. Therefore, the various experiments believed to have proven vitamin-A deficiency were so blatantly flawed that anyone’s grandmother could have told them that they had gotten it wrong. The experiments just do not pass the litmus test of common logic, and they most certainly cannot stand up against even the most trivial amounts of critical thinking.
In other words, these early scientists failed to ask the very most basic and fundamental questions. Biologically speaking, and in an evolutionary context, how is it possible for us to be here? One winter would have wiped out nearly all of these species, and us, from the planet. Seriously, can you imagine the skin and eyes disintegrating, burning off in mid-winter, weeping lymph fluid and so easily becoming infected, in just eight weeks, and yet these species have survived, and survived very well over tens of millions of winters? Talk about missing the obvious.
What I know from my early years growing up on the farm, is that rats can winter for at least nine months, living on nothing but grain, and do very, very well. Rats do extremely well for nine months, or more, without a single molecule of vitamin-A in their diets. They have perfect vision, and remain in great health. The bigger ones can grow to be about a third the size of a house cat. They have high energy levels, and vigorously and ferociously defend their territory. They reproduce, well like rats, too on their vitamin-A deficient winter diets. But, don’t take my word for it, just ask any prairie grain farmer if a rat can live all winter long on grain alone. Therefore, a simple grain farmer could have so easily debunked all the ridiculous vitamin-A deficiency theory from the esteemed academics in a matter of minutes. It appears that these academics had a complete disconnect from nature, reality, and sensible logical thinking too. With these very basic and obvious facts the entire premise of vitamin-A deficiency is nothing more than a complete myth. It is simply impossible, except for possibly in the most ridiculously long term and extreme periods of starvation. But, what you’ll soon learn is that animals, and humans, will die of starvation before they are truly vitamin-A deficient. In other words, both animals and humans will die first due to prolonged starvation before the eyes fail. Once again, from an evolutionary point of view, this is perfectly logical too. The body needs to maintain the eyes and vision to the very end of life.
So, where and how could these early researchers have gotten it so incredibly wrong? That’s the question we are going to investigate here. We are going to reopen the cold case of the very determination of vitamin-A being a vitamin at all. The surprising truth is that vitamin-A is not even a vitamin at all. No, it is a complete myth based upon bad science. So-called vitamin-A is simply far, far more of a toxin than being a vitamin. The sad truth is that it is a toxic molecule that has now killed tens of millions of people, and that’s just in the last few decades. Additionally, there are more than a 100 million people in North America who are now the walking wounded due to its insidious destruction of our epithelial tissues and associated organs. What you are also going to learn is that the names given to the chronic diseases simply hides the fact that most of them are really the same disease. They are the same diseases because they are all diseases of one tissue category; it’s the epithelial tissues. The names of the chronic diseases are obfuscations, and are pretty much meaningless labels. To make the point perfectly clear, consider the following: diabetes is a disease of the pancreatic epithelial tissues. Eczema is a disease of the skin, a stratified epithelial tissue of the epidermis. Heart disease and stroke are diseases of the epithelial tissues lining the blood vessels. Multiple sclerosis is a disease of the epithelial tissues making up the myelin sheaths wrapping nerves. IBD, Crohn’s, and colitis are diseases of the epithelial tissues making up the lower digestive tract. Cataracts is the disease of the epithelial tissues making the lens of the eye. Xerophthalmia (chronic dry eyes) is the diseases of the epithelial tissues of the tear ducts, and other glands within the eye. Asthma is a disease of the epithelial tissues of the lungs. The same applies to many of the other named chronic diseases. They can be more appropriately, and correctly, named as epithelial disease. However, we need to be a bit more precise; they are truly epithelial poisonings. There is only one potential poison in our foods that can be responsible for all of this, and it is vitamin-A!
Once again, the incredible irony here is that vitamin-A does not protect from xerophthalmia as claimed by the experts in ophthalmology and the World Health Organization; rather it causes xerophthalmia, and amazingly cataracts too. Almost unbelievably, these self-proclaimed experts, and proponents of vitamin-A supplementation, have got it completely, and perfectly, backwards. If any ophthalmologist happens to read this, the truth is that vitamin-A is causing the destruction of the vision in tens of millions of people around the world. You should be concerned about that. If you think I am wrong and are up for a large wager, I’m in.
Also, if you happen to be wondering why I’ve used an 11-point font in this e-book it is because I know that my intended audience, mostly people with autoimmune diseases, will need the larger font size.
What we are going to do in the next few chapters is to go on a deep dive into the evolution of the very discovery of vitamin-A. From there, we are going to carefully investigate the subsequent follow-on vitamin-A deficiency theory, and it’s supporting experiments. As we undergo that investigation you’ll see that we enter a bit of an alternative universe where things are often the inverse of reality, scientific “facts” are almost fabrications from vague, confusing, and totally conflicting experimental results. The evidence I am going to present in the subsequent chapters leads me to firmly believe that vitamin-A is not a vitamin at all. As I’ve stated above, it does not belong on the list. It is an imposter. I believe that it is simply nothing more than a poison. If I am correct about this, it will be a case where science has not only gotten it completely wrong; it has gotten it perfectly backwards too.
Of course, this is no harmless little scientific blunder. Rather it has been catastrophic for human health worldwide. By giving the prestigious vitamin designation to a highly toxic molecule and its subsequent supplementation into our major foods has resulted in the mass poisoning on an almost unbelievable scale. The resulting death toll is easily now in the tens of millions, and 100s of millions are now chronically diseased because of it (no drama intended, it’s just the facts).
The early part of the 20th century was the heyday of the discovery of vitamins. In the late 1890s, there was the evolution of the concept a vital, yet hidden, essential substances in our foods. In addition to the proteins, fats, and carbohydrates that were well known, researchers had concluded that there were other special components needed for human development, growth, and sustained health. Without these hidden substances, serious deficiency diseases would develop. Originally, these hidden substances were called “vital amines,” and thus the subsequent abbreviation to vitamins. The earliest classification of these vital components were divided into two categories, the fat-soluble A’s and the water-soluble B’s.
In the early 1900s investigators went on an exploratory expedition to isolate and determine what these special food components, or “factors,” were. Of course, with the discovery of these components came the potential for great academic recognition, prestige and possibly even the financial rewards in the form of Nobel prizes, and patents, etc. Therefore, these early researchers were highly motivated to make discoveries. The earliest, and the first fat-soluble vitamin, to be discovered and isolated was vitamin-A.
One of the first thought to be indicators of deficiency of the vitamin-A was the condition of night blindness. Now, it’s very important to understand what is meant by the term of night blindness. It is not actually being blind at night. It is the condition of the slow adaptation to darkening light conditions. To this day, it is still this slower adaptation to changing light conditions that is measured in determining the severity of vitamin-A deficiency. Therefore, night blindness is not a condition in the deterioration of the photoreception capability of the eyes.
Some of the early (circa 1900) well documented and most widely published examples of night blindness were in the Newfoundland fishermen. After being at sea during the day, with the eyes exposed to the glaring sunlight off the water, many of the men found it very difficult to adapt to the diminished light conditions as night fell. This night blindness condition was not only problematic but quite dangerous too as the fishing ships sailed back to the rocky shores. But, the night blindness condition was usually somewhat resolved by a good night’s sleep. Therefore, night blindness was not at all permanent damage to the eye.
Of course, the crafty and resourceful Newfoundland fishermen improvised effective workaround solutions to the problem. One solution was to wear a patch over one eye one day and then alternate the patch to the other eye the next day. Each day, as night fell, they would remove the patch, and they’d have reasonable night vision from the previously covered eye. Not surprisingly, this was a well-known technique used by pirates for decades before then too. However, for pirates, the motivation was not for the safe return of their ship to shore at night. No, for pirates, the quick adaption to low light condition was an essential life survival and battle skill. When they boarded, and raided other ships, and went below deck, they would be at a clear disadvantage to the well low-light adapted and sword wielding defenders.
In addition to wearing a patch on one eye, the Newfoundland fishing ships adopted a similar measure, where they would keep one crew member below deck all day long, and this designated crew member would then be brought up on deck upon nightfall to safely navigate the ship back to shore. But, the craftiness of the Newfoundlanders did not stop there. They also learned that if they dripped some cod liver oil into the eyes at night, it would accelerate their recovery to good vision by the next morning. There are many similar accounts in the writings from antiquity of using liver oil applied directly into the eyes to aid in the recovery from night blindness as well. There are of course accounts of consuming liver, or just the liver oil, curing night blindness too. But, the condition of night blindness was only one, and the far more minor one, of the conditions ascribed to the suspected vitamin-A deficiency. The other far more serious disease conditions were prolonged dryness of the eyes, the dryness then spreading over the cornea, subsequent scarring, lesions, and eventually significant degeneration of the eye. This spectrum of the disease conditions is termed: xerophthalmia.
As these more serious conditions progressed, the disintegrating tissues almost always became infected. If the condition were not remedied it would ultimately lead to complete, and irrecoverable, blindness. From these accounts, the early vitamin researchers logically concluded that there must be some special hidden factor in cod liver oil that was so beneficial to the eye in promoting the recovery from night blindness, dry eyes, and even quick healing of the lesions.
However, very early on there were clearly flaws showing up in the grand theory, but they were completely ignored or glossed over. One very important bit of information the early researchers failed to appreciate was the fact that Newfoundland fishermen also ate codfish nearly every single day. It was the staple protein, if not the primary food in the region’s diet for like 400 years. With that knowledge and two minutes of clear thinking, they should have probably concluded it was not even possible for it to be a deficiency condition at all. What was far more logical, and completely obvious even at the time, and what any self-respecting pirate could have attested to, was that it was the overexposure to sunlight that caused their night blindness. But, the problem for these researchers with that position is that you can’t make great discoveries, and there’s no money to be made, without finding a special deficiency. Therefore, to rationalize how the dripping of cod liver oil into the eye was getting the vitamin-A into the cells of the eye, they concocted this bizarre scenario of the liver oil running backwards in the (likely blocked) tear ducts, down through the nasal cavities, into the throat, down through the digestive tract, then into the blood, through the liver, released back into the serum, and then back up into the eye. Once into the eyes, the essential vitamin-A factor did its magic of repairing the condition of night blindness, and it did it in just eight hours. Damn, isn’t that brilliant! But, let’s not fault just the early researchers in this fabrication, because, the same accounts and illogical reasoning is parroted in modern scientific literature too.
One much earlier experiment, from around 1816, particularly stands out for me. A researcher named François Magendie put dogs on a starvation diet of just sugar water. Sure enough, within just four weeks, the dogs started to develop eye lesions. Damn! It was almost conclusive; it must be a vitamin-A deficiency (not B, not C, not D, nor proteins, nor fats, nor minerals, etc.). Of course, this is a completely unnatural diet for a dog. When in all of evolutionary history have dogs ever consumed sugar water? It is about as logical as using a diet of water and peach pits to prove vitamin-A deficiency. Even though these dog experiments were done way back in the early history, they too are still cited in contemporary, and current medical textbooks as evidence of vitamin-A deficiency. Of course, this ridiculous dog diet proved no such thing as vitamin-A deficiency. If nothing else, it simply proved the toxicity of sugar in the diet. Naturally, anyone with even a little experience with animals in the wild knows that animals don’t go blind in just four weeks even due to starvation. Once again, if that did happen, then the species would not even be here at all. Other species, such as the wolf, quite routinely do starve for much longer than four weeks, and their vision remains perfect. Of course, these very early experiments of sugar water diets are incredibly unscientific and are clearly almost senseless. Admittedly, they are only early starting points in the vitamin-A deficiency investigation. Yet, similar bizarre extrapolations continue to this very day to support the vitamin-A deficiency theory.
Before we move on, we need to understand some of the terms used to describe the various conditions and diseases of the eye. The more broadly used, and encompassing term, is “Xerophthalmia.” The simplest definition of Xerophthalmia is the condition of “abnormal dryness of the conjunctiva and cornea of the eye, with inflammation and ridge formation, typically associated with vitamin-A deficiency.”
Here’s a short glossary of some of the other related terms we’ll come across.
Bitot’s Spot - are the buildup of keratin located superficially in the conjunctiva of the eye. They are thought to be a key indicator in the diagnosis of vitamin-A deficiency.
Conjunctiva - the mucous membrane that covers the front of the eye and lines the inside of the eyelids.
Dermatitis - is a general term that describes an inflammation of the skin.
Keratomalacia – the softening and progressive disintegration of the cornea of the eye. Thought to be an indication of the more advanced stages of vitamin-A deficiency.
Night Blindness – impaired ability to adapt to low light conditions, or being temporarily blinded by bright lights at night. Thought to be a major clinical indicator of vitamin-A deficiency.
Ophthalmia – inflammation of the eye, especially conjunctivitis.
Retinol – the simple chemical name for what’s called pre-formed vitamin-A.
Ulcer – an open sore that has occurred without externally induced trauma.
Xerosis – generally means drying of the tissue, often used in the context of the condition of the eye.
| Table 1 Classification of Xerophthalmia conditions | |
| Condition | Code |
| Night blindness | XN |
| Conjunctival xerosis | X1A |
| Bitot’s spots | X1B |
| Corneal xerosis | X2 |
| Corneal ulceration (keratomalacia) < 1/3 corneal surface | X3A |
| Corneal ulceration (keratomalacia) = 1/3 corneal surface | X3B |
| Corneal scarring | XS |
| Xerophthalmia fundus | XF |
| Source: The WHO 1981 | |
The dry eye condition usually originates with the decreased production of mucus or tears. The mucus or tears are of course critical in keeping the eye lubricated, and it also helps protect against infections. However, as the dry eye condition worsens, and more tissue structures and surfaces become involved, it can develop into very serious eye disease. There is a spectrum of such conditions. Each one is uniquely named, ranked, and categorized according to severity. Somewhat confusingly, the entire spectrum is included under the umbrella term of Xerophthalmia. Maybe a bit oddly, even though Night Blindness is not a condition specifically of dry eyes, it too is included within the Xerophthalmia classification spectrum.
Now, it is very important to understand the conflation between the terms “xerophthalmia” and “vitamin-A deficiency.” The two terms are almost completely synonymous. The theory and belief, that vitamin-A deficiency causes all of the above conditions is so entrenched and ingrained in medical thinking; the two terms are nearly inseparable. So much so, that there’s an almost circular dependency between them, each term is used as an indicator of the presence of the other. Meaning, the presence of “xerophthalmia” is a measure of the “vitamin-A deficiency” in a population. And conversely, therefore, the degree of “vitamin-A deficiency” in a population is measured by the incidence rates of any of the “xerophthalmia” spectrum conditions. Okay, with that bit of terminology covered, we can move on here.
The next suspicious aspect in the evolution of the deficiency theory was that there were other early researchers who were showing that just having adequate amounts of dietary fats, and especially that of butter fat, could prevent and reverse the same “xerophthalmia” disease conditions of the eye.
Probably the most noted was the work of Dr. Masamichi Mori in Japan (not to be confused with S. Mori of Wisconsin who is another prominent early vitamin-A researcher). In 1904, Dr. Masamichi Mori provided a comprehensive account of the pathogenesis of the Hikan condition he observed in children in his clinic. The term Hikan is the Chinese name for these same diseases of the eye. There are some very important clues and information that Dr. Mori provides us in his report. Firstly, the disease condition occurred mostly in younger children, from ages 1 to 4½ years-old. Therefore, somehow younger children were more susceptible. Secondly, is that the condition was occurring more frequently in boys, at a ratio of about four boys to three girls. The next and the critically important observation made by Dr. M. Mori was that this disease was not at all limited to just the eyes. By Mori’s observation, and definition of the disease, it included five distinct symptoms (comorbidities if you prefer that term). These were: diarrhea, abdominal expansion, excessive appetite, night blindness, xerosis of the conjunctiva, and thinning of the hair.
In addition to these five specific symptoms, he also documented the children commonly having dry skin, and having significant sensitivity to sunlight too. One other very important little detail he documented was that the condition was more prevalent in the summer months. Therefore, clearly, the Hikan disease condition was much more than just an eye disease. Nonetheless, Mori very successfully treated the disease by just adding more fats to the diets of the children. He was quite certain that it was just the additional fats and not something special hidden within the fats, that was responsible for the recovery from the disease. But, to Mori’s American contemporaries, and modern day historians, their conclusion was that Mori had missed the mark with his hypothesis and that it was not just the additional fats that had ameliorated the disease.
However, what I hope to show you later, is that Mori was indeed correct. It was not some deficiency condition ailing these children at all. Rather it was a poisoning, and the additional butter fat in their diet was emulsifying and therefore protecting them from it.
Now, it is very important for us to remember Mori’s documented comorbidity pattern:
- more common in boys than girls
- the younger the child, the more susceptible they are
- diarrhea
- abdominal expansion
- excessive appetite
- night blindness
- xerosis of the conjunctiva (dry eyes)
- thinning of the hair
- dry skin
- sensitivity to sunlight
The reason that it is important to remember this pattern is because we need to be able to recognize it again when presented in another context in a later chapter.
Next, in 1909, W. Stepp in Strassburg was conducting experiments on mice deprived of fats in their diets. He concluded that diets of just proteins, carbohydrates, and inorganic salts were not sufficient in sustaining life. However, as with M. Mori’s work, Stepp’s American counterparts made the determination that it must have been some hidden missing factor in the fats, and therefore it was a deficiency that caused the animals to become ill and die.
Naturally, there are other similar reported accounts from this era of fat deficiencies causing night blindness and xerophthalmia. Yet, these reports did not dissuade the vitamin-A deficiency theorists. The clincher study thought to have cracked the case in favor of the deficiency theorists is probably the work published by Bloch in around 1912. Bloch was a pediatrician working in Demark and was treating eight children with xerophthalmia. It is quite an interesting report because there are two distinct groups of children, those that get fat milk, and those that get fat free milk. Half of the children on the fat-free milk developed night blindness, and xerophthalmia. Of special note, like in M. Mori’s report, these children are very young, 1 and 2-years of age, and they also exhibited sensitivity to sunlight. Likewise, Bloch reported that the onset of the disease condition in the children occurred almost simultaneously in the months of May and June (when there’s more sunlight). Bloch treated the affected children with cod liver oil, and within just one week they had made remarkable recoveries. Once again, this recovery was attributed to the vitamin-A content in the cod liver oil, and therefore, it was concluded that it was the addition of vitamin-A that was the responsible curative agent, and not necessarily the oil itself.
So, with these studies, the researchers were zeroing in on the vitamin-A component so abundant in cod liver oil and to a lesser extent, in butter. Since it sure looked to be the case, they quickly assumed that it was responsible for accelerating the recovery and curing the children of the night blindness condition. Of course, they very logically assumed that conversely, a deficiency in vitamin-A would, therefore have, have caused the conditions to develop in the first place.
At the same time, the early American researchers quickly sped ahead and started conducting many more experiments on animals to prove their vitamin-A deficiency theory. By using vitamin-A deplete diets in their experiments, they quickly induced the xerophthalmia conditions, and many other severe conditions, in their lab animals. They claimed that the only significant missing nutrient from the animal’s diet was vitamin-A. Therefore, they felt that they had isolated it down to the disease being solely attributable to a vitamin-A deficiency. With that extrapolation, the blame, and root cause of night blindness, and the many assumed to be associated other diseases of the eye was pinned squarely upon a deficiency in vitamin-A.
From that presumptive observation, we all quickly fell into the cascading pit of failed and catastrophic so-called scientific investigation that led to the determination of vitamin-A being a vitamin. Looking at this evidence, and I suppose just due to our historical human conditioning, the thinking was that it just had to be a deficiency and not a toxicity condition causing the disease. In a strange way, this assumption of deficiency prevails even today. What I see today, is that almost everyone believes that when they get sick (and when clearly not due to infections), that they must be deficient in something.
Thus, by 1913 it was conclusive, the vitamin-A deficiency condition was proven as the cause of both night blindness and the more serious disease conditions of xerophthalmia and conjunctive xerosis. This conclusion then officially puts vitamin-A as the first vitamin on the list to be confirmed. The credit for the discovery of vitamin-A goes to the American researchers Elmer McCollum and Marguerite Davis. In 1913, it was simply called fat soluble A, and in 1920 it gets renamed to the more official and prestigious term “Vitamin-A.” However, McCollum’s legacy in this matter is not limited to just being given credit for the discovery of the vitamin. He also defines the official experimental lab diet that nearly all subsequent researchers use to replicate his results. With that bit of historical background, now here we are, over 100 years later, undertaking some forensic work to determine if they might have gotten it completely wrong.
Naturally, there have been far more rigorous, and scientifically conducted experiments in the 1920s, ’40s, and even the 1960s that are used to seal the deal, close the case, and put the question of vitamin-A deficiency to rest for once and all. However, there is a wickedly deceptive flaw exhibited in almost all these experiments. It’s hidden in the McCollum designed diet. In addition to the critical scientific flaw in their experiments, there other humanistic factors that prevent them from seeing that something is drastically wrong and completely illogical in their results.
The first major humanistic factor is their certainty about it. These early researchers are so certain that they’ve conclusively proven the case it makes them blind to what should have been obvious all along. The second major problem was that they failed to accept and appreciate that they were probably working with incomplete information.
We’ll investigate these follow-up experiments in a lot more detail in a subsequent chapter. For now, we just need to know the stated conclusions and interpretations made from them. Basically, and a bit simplified, it was that both animals and humans have the same almost razor thin tolerance for vitamin-A deficiency. Get too little of it, and you’ll go blind, or you’ll first go blind and then you’ll die; or get too much of it and you’ll die with your skin painfully burning off. Either way, it’s a dicey balancing act.
Yet, somehow these early researchers, and even researchers today, have completely ignored the fact that animal and human history is full of prolonged periods of complete starvation with no such “deficiency” lesions developing in the eye, and of course no blindness either. But, with fame and glory on the line, there’s not much time or effort allotted by these researchers to such logical thinking. Therefore, it was a vitamin-A deficiency, done deal, end of the story, let’s move on to filing patents, and making money. I’d like to say that these folks presented a lot of scientific arrogance in this endeavor. But, somehow, I don’t think that was the case. I think they were just too caught up in it, and therefore they failed to see that something was hugely amiss.
Either way, what you’ll soon find out, is that these so-called definitive experiments were completely botched, and almost as ridiculously flawed as this sick experiment with dogs on the sugar water diet. One source of the problems is that trying to design a viable, yet vitamin-A deplete, diet to experiment with is surprisingly rather tricky. The thing is, almost all foods on the planet have at least some vitamin-A in them. In other words, to come up with a completely vitamin-A deplete diet, you need to rule out so many other needed nutrients at the same time. But, that’s only the start of the problems introduced in these experiments. There was an unforeseen, and amazingly ironic, little unknown that secretly tipped the scales.
Before we dig deeper into the mysteries of vitamin-A deficiency, we need to back up a few steps and talk about how experiments fit into science and the basic rules of the scientific method. Even if you are familiar with this topic, please don’t skip this chapter, as it sets up some context needed for the subsequent chapters.
The “experiment” is one of the most critical cornerstones of science. The experiment is used to prove or disprove a theory. Before theories are tested with experiments, they are generally put forth as a hypothesis. As a hypothesis is being refined, and if it gains some strong supporting evidence it progresses to being called a theory. Only after hundreds of repeated experiments, yielding exactly, or very close to exactly the same results, and the experiments are conducted by many different scientists, and preferably from around the world, can a theory be regarded as a fact.
In addition to the “experiment,” the other cornerstones in science are what are called the pure sciences of mathematics, physics, and chemistry. Sometimes, they are referred to as the “exact” sciences. They are called this because they usually provide exact answers to questions and problems. Although they are referred to as being exact sciences, that does not in any way connote that they are complete sciences. It’s far from it, most scientists in these fields realize just how little they know. They are usually humble, and they know that they are never working with the complete picture. However, what they do know about, they are reasonably certain that it is correct. Even with that, there are sometimes complete upsets in the “exact” sciences. The current new discoveries being made in the world of quantum physics is a good example. How are these upsets proven? It is with the discovery of new information and then having it backed up by additional experiments.
There are other fields of science that are considered “inexact” sciences. A good example is geology. Geology is more appropriately called the science of concepts and related processes. These concepts are mostly “provable” via observations of the present processes in nature, and the extrapolation of them back through the millennia. Although geology is a wonderful science, it is far from exact, and it is often difficult to design experiments to conclusively prove geological scientific facts. Nonetheless, one of the most important lessons we can use from geological sciences is the concept of very slow processes applied over very long periods of time yielding dramatic results.
Further down the spectrum of the “exactness” scale of the sciences would be many of the medical sciences. Biological systems are amazingly complex and we only truly understand a very tiny fraction of what remains to be learned. Even further down the spectrum, would be the so-called sciences of mental health and psychology. Currently, these fields are anything but science. They are simply speculations, and guesses or hunches as to the real functioning of the human mind and the brain, at the very best.
When designing, and conducting experiments, there are a few golden rules that need to be followed. Firstly, the experiment must be completely repeatable. The results must be reliably measurable. When the experiments are repeated by others, they must yield exactly (within the margin of acceptable measurement error) the same results. If an experiment fails to meet these criteria, then it is deemed to be invalid. In other words, it probably proves nothing. If an experiment yields significantly varying results, then the experiment is not well designed. The scientist then needs to determine why the results are not consistent, and refine the experiment to narrow down, and eliminate, the source of the differences.
The second golden rule in experiments is to change only one variable at a time. If an experiment has two or more variables changing at one time, it can be very difficult to claim the outcome proves the effect of either one independently.
The third golden rule in experiments is to objectively observe, and see what you are looking at. There is no room for biases, or for manipulating the data to have it ultimately “prove” the result you are looking for. Manipulating the data, A.K.A. cooking the books, is called scientific fraud.
The final, and the most important, golden rule is that if the result of well designed, and valid experiments fails to support a theory, then the theory is very likely wrong. Although this can be frustrating, and disappointing, legitimate researchers must always accept the results as a fact. Just to repeat it: the critical point here is that if a well-designed and valid experiment fails to support a theory, even once, or even apparently just one time, then the theory is wrong.1
But sometimes even “failed” experiments can be hugely valuable. This is because when conducting an experiment to test a theory, and even though the experiment fails, it may reveal some other completely unexpected and intriguing results. Many major discoveries in science have indeed been made when conducting “failed” experiments that were in completely unrelated fields. Some notable examples are the discovery of microwaves from radar research inducing heat in food leading to the development of microwave ovens. Likewise, some of the major pharmaceutical drugs in use today were discovered by lab mistakes made in the textile, and fertilizer industries.
Therefore, to be a legitimate and successful scientist one needs to recognize that science is never complete, and you must always remain open-minded. What’s accepted as being the truth today could be overturned with new evidence tomorrow. You must always remain ever curious and be on the lookout for anomalies, even the tiny ones that appear completely insignificant to most other people. You must always have your eyes open and see what you are looking at. So often people fall into the trap of seeing only what others are telling them they are looking at.
So now, why did we need to review the background rules on conducting experiments? It’s for two primary reasons. Firstly, it is because we are going to analyze and review the early experiments used to “prove” the vitamin-A deficiency theory. Using these very basic rules you’ll be able to gauge the validity of those experiments, and that of the conclusion drawn from them.
The second reason for reviewing the ground rules for conducting experiments is because it will soon be your turn to be a scientist too. Don’t worry, you don’t need to have a background in science, or mathematics, etc., because anyone can conduct an experiment. I am going to ask you to conduct a trivial and fun little experiment with a few small animals such as gerbils, hamsters, or pet mice or rats. Although it will be a trivial, fun, and small experiment, when your results are combined with others who are conducting effectively the exact same experiment, it could be one of the most important experiments in human history. Also, don’t worry, no animals will be harmed. Of course, I’ve already conducted this small animal experiment, and I have my results. However, as I’ve stated above, the results from one person are not at all good enough. Therefore, I am asking you to be one of hopefully thousands of other people from around the world who do the same experiment and for you to contribute your results.
This is the fantastic thing about science. All the theoretical debates can’t hold a candle to the experiment. The experiment trumps the debate. The experiment is king! The experiment quietly cuts through even the loudest rhetoric, and regardless of who’s shouting it, and proves or disproves the theory. Obviously, this is not to say that critical and logical thinking isn’t just as important as the experiment. On the contrary, critical and logical thinking is extremely important. Thus, the experiment is in no way a replacement for critical and logical thinking; rather it complements it.
With that, by conducting a fun little experiment, and applying your own critical thinking, you’ll get to verify and see the results with your own eyes. Therefore, you don’t have to, and you never should just take someone’s word for it. Even though I’ve tried to back up every major statement and claim I make in this e-book with references, you most certainly should not just take my word for it either. At the very least, you should check and analyze those backup references. My interpretation of those referenced studies could be quite different than yours, and my conclusions might be entirely different too. Although I believe I am correct, I am still open minded too. I know I could be wrong. But, it does not matter if I think I am right or wrong, and it does not matter if you think I am right or wrong. What matters is that you help prove it one way or the other. What really matters here is that you conduct the experiment. You get to do it quietly with no outside influences, and therefore with no one’s thumb secretly tipping the scale so to speak.
Now, regarding the theory of vitamin-A deficiency, this is absolutely great because you get to participate in (potentially) overturning one of the most fundamental and longest held beliefs in modern medicine. I believe it also just happens to be the very root cause of most of the chronic diseases we are dealing with in the Western world too. Come on; you can’t resist being part of that, can you?
Even though we are investigating the theory of vitamin-A deficiency, we need to have a good understanding of the opposite side of that coin; that of vitamin-A toxicity. The primary reason we need this information is that we’ll have a much better understanding of the results from the vitamin-A deficiency experiments. That’s correct, knowing what to expect in the vitamin-A toxicity scenario will enable us to recognize what was really being demonstrated in the early vitamin-A deficiency experiments.
One of the most important aspects to fully understand and appreciate about vitamin-A toxicity is that it affects the entire body. It does not affect just one organ or show up in just one tissue type. No, the scope and breadth of the destruction it will cause is just staggering. It will slowly destroy everything from the hair on top of your head down to the nails on the ends of your toes. It will also slowly destroy every other organ and tissue in-between. Although vitamin-A toxicity will be most aggressively expressed by the destruction of the epithelial tissues, it will have profound and devastating cascading effects throughout the rest of the body too. Vitamin-A is very capable of destroying every cell in the human body. However, it’s most devastating effect is upon the body’s stem cells. Although most of the visible toxicity destruction takes place on the surface tissues, that of the skin, eyes, hair, and joints, that is just the beginning of its reach. It will slowly suck calcium out of the bones and teeth. It will distort the very shape of the spine and skull. It will be correspondingly destroying all the internal organs too. It will destroy the pancreas, the lungs, the kidneys, the digestive tract, the liver, the spleen, the thyroid, the lymph nodes, both the female and male reproductive organs, all mucus generating tissues, all villi structured tissues, the blood vessels, the heart valves, the eyes, the ear canals, and more. As the scope of the toxicity destruction progresses, it will seriously impair the functioning of the brain too. As the bones are slowly depleted of their calcium, that calcium reacts with the iron and oxygen in the blood. That exothermic reaction then not only causes intense inflammation, it drastically reduces and limits the blood’s ability to carry adequate amounts of oxygen. That limited oxygen supply then, in turn, can most certainly cause chronic fatigue, depression, psychoses, and even long-term brain damage.
Yes, all this destruction can be caused by getting too much of what modern medicine has termed, and wants you to continue to believe, is a “vitamin.” To me at least, that is one wicked sounding vitamin. Of course, with what I’ve just described, you should now be asking, if vitamin-A can be so toxic, why are we not all dead? Well, the two biggest variables here are just dose and time. Another big factor is that the human body is extremely well adapted to dealing with this toxin on a somewhat daily basis, but in reasonable amounts. Now, what’s happened is that our average daily consumption of this toxin has exceeded, and gone way past what’s historically been reasonable. Additionally, there’s a third important factor, and that is that retinol is a bit of an opportunistic toxin. If cells are protected with strong and integral fatty membranes, it is not going to easily get inside of them to where it can cause damage. So that, in a nutshell, is how and why we are now being slowly poisoned by it. Even though we are not all dead, at least half of us are now indeed mysteriously sick.
Naturally occurring forms of vitamin A include retinol, retinol esters, retinal and retinoic acid. The alcohol form, retinol, predominates in the circulation but it is too toxic for storage. Instead, the liver stores retinol as retinyl esters - principally palmitate.
Of course, there’s much more to this toxicity story. Another hugely important part of the story is that vitamin-A is a fat (lipid) soluble molecule. Therefore, it will naturally be absorbed (emulsified) by fats. This includes both dietary fats, and the body’s storage fats. For us, most of the storage of vitamin-A is in the fats within the liver, and to a lesser extent in the fats of the adipose tissues (the skin etc.) This storage ratio is not constant over time. As the liver becomes more and more saturated, more vitamin-A will remain in serum longer and slowly seep into and accumulate within the lipids of the adipose tissues.
Even with that, the vitamin-A stored within these fats is not yet toxic. In the early going, it is safely wrapped up, and therefore does not get rapidly exposed to cell membranes. Somewhat similarly, vitamin-A can be safely transported in serum within wrapper proteins. These wrappers are called the retinol binding proteins, the RBPs. When encased within the RBPs, no part of the vitamin-A molecule is exposed to the outside world. In this packaging, it is once again safe, harmless, and maybe even useful.
So, vitamin-A in reasonable amounts, given adequate amounts of dietary fats and proteins, is by itself not too terrible. However, there is a tipping point to where vitamin-A can, and does, easily convert into an extremely nasty, and highly toxic molecule (and the thought to be active form of the vitamin). This converted vitamin-A molecule is called retinoic acid. Retinoic acid is so incredibly toxic it is used as a chemotherapy drug. The reported functioning mechanism of the “drug” is that it quickly kills replicating cells.
However, it is critical to understand that every cell in the body will convert excess vitamin-A into retinoic acid. The overall rate of conversion is proportional to the number of cells that are exposed to the vitamin-A molecule. I believe it’s also proportional to the number of cells with damaged cell membranes. Therefore, to be safe, there should never be any excess vitamin-A in the body. What does excess vitamin-A mean? It means several things. One is that you never want to consume vitamin-A at a rate that exceeds your body’s safe storage rate. What’s your safe storage rate? It’s highly variable, and individualistic too, but it will depend mostly upon your current storage levels. The storage levels are dependent on not only our body’s lipid levels, but the composition of those lipids, and the current concentration of vitamin-A within those lipids. As we start to exceed the vitamin-A load carrying capacity of those lipids, we will move into the toxicity state. But, not only is the body well prepared to deal with vitamin-A, it is going to adapt in real-time in response to the potential threat. Our body is ultra-smart. It is going to force us to become fatter. Getting fatter is needed to protect us from the potential toxicity of having the vitamin-A molecule exposed to cell membranes. The body is also going to grow our liver larger, and larger, and larger too. But, as with most systems, there are limits. Once we approach these limits, more and more circulating vitamin-A will be exposed to cells, and the subsequent normal processes of converting vitamin-A to retinoic acid will take place.
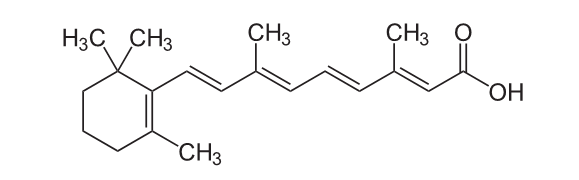
It will start slowly, once cell at a time, and one molecule at a time. However, as more vitamin-A becomes exposed, the process will accelerate. Once again, the real big risk here is the conversion of vitamin-A to retinoic acid. Retinoic acid has about ten times the toxicity of vitamin-A (retinol). That is not to say that vitamin-A is not toxic. It is just not immediately toxic because it takes time to convert into retinoic acid. To better understand the relative toxicity between these two molecules, retinoic acid is by far the more toxic one. But, the conversion from vitamin-A (retinol) to retinoic acid is just a simple oxidation reaction. All that’s needed for the reaction to take place is a little activation energy and oxygen.
Retinol (vitamin-A)
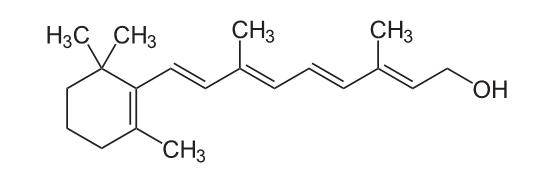 |
simply picks up the extra oxygen atom on the end of the side chain to become Retinoic Acid.
 |
Vitamin A and the carotenoids are sensitive to oxidation, isomerization, and polymerization when dissolved in dilute solution under light and in the presence of oxygen, particularly at elevated temperatures.
Health, Survival, and Vision
Alfred Sommer and Keith P. West
With James A. Olson and A. Catherine Ross
Oxford University Press, 1996
ISBN: 9780195088243
See: page 223
Therefore, since the conversion of retinol into retinoic acid is so simple, we can think of vitamin-A as just being the devil in disguise. The true sinister identity of retinol is only revealed after it has metabolized into retinoic acid. The takeaway here, and what’s critically important to remember is:
Retinol is metabolized to retinoic acid in normal cells.
The natural metabolism of retinol into retinoic acid is very well known and widely documented. It is confirmed here in this excellent 2006 report titled: The acute and chronic toxic effects of vitamin-A.2
The A postprandial increase in serum retinol concentration may be blunted when vitamin-A is ingested with either food or ample dietary fat, whereas a significant amount of free (unesterified) retinol may circulate when vitamin-A is consumed without dietary fatty acids, which leads to excessive production of retinoic acid.
Source: The acute and chronic toxic effects of vitamin-A1–4, Kristina L Penniston and Sherry A Tanumihardjo
Therefore, depending upon a person’s particular storage situation and dietary intake scenarios there may be periods of time where excessive amounts of retinoic acid are produced. This has of course been directly confirmed in experimental studies.
Once again from the report on the acute and chronic toxic effects of vitamin-A.
An acute elevation of retinoids other than retinyl esters — eg, retinoic acid — occurs after the ingestion of a large amount of vitamin-A, possibly because the intestinal absorptive capacity is overwhelmed, which leads to the oxidation of retinol to retinoic acid by the intestinal enterocytes (30) and to the rapid formation of retinoic acid from retinol in certain cells (5). Whereas retinoic acid can be produced from excentric cleavage of beta-carotene in humans (31), it is generally considered a minor contributor to circulating concentrations, at least in normal, healthy persons.
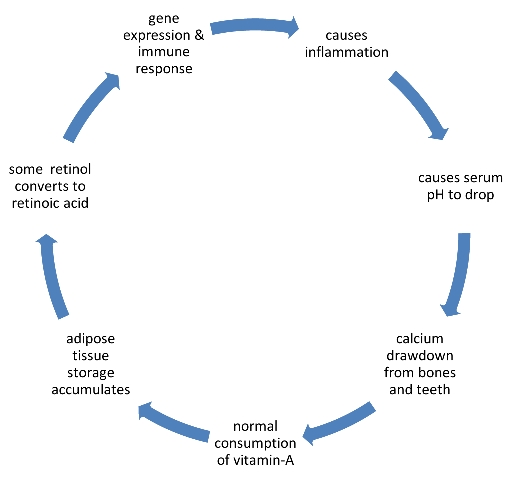
Figure 1 The trapdoor Retinol consumption cycle
|
Therefore, the overload of vitamin-A consumption is a trap. The trapdoor loop looks like this:
Once you near your body’s storage capacity, and or the storage rate capacity for vitamin-A, all kinds of horrible things will start to happen. You’ve now fallen through an almost one-way trapdoor. There’s no known antidote, as far as I know of. So, with that, you’d think that the vitamin-A researchers, both the folks from the 1920s, ’30s, etc. and the modern day current so-called experts in the field would have realized the vital importance of getting it right. Given the dire consequences of getting it wrong, they should have been incredibly careful and gotten this whole vitamin-A dependency, and deficiency, theory exactly correct. It should have been verified, and re-verified at least a thousand times over, leaving absolutely no room for error. But, no, that did not happen.
So now, what’s the danger in getting into this elevated storage state? Well, it too is proportional, and highly variable. But, in small measure, or large, a dose of a chemotherapy drug can’t be a good thing to be dealing with on a repeated basis. When there is retinoic acid in serum, or in the intercellular fluids, there is sure to be cellular damage. Where’s this cellular damage going to happen most often? Well, once again it is going to be variable, and it depends, and it might be almost random. But, it is clearly going to most commonly show up in the eyes, and the adipose tissues, such as the skin.
The reason retinol and retinoic acid are so incredibly toxic is because being hydrophobic it easily slips through the cell’s fatty outer and nucleus membrane structures. From there the molecule’s cyclohexane group is a perfect fit into the cell’s RNA molecule.3
 |
The perfect fit allows the retinoic acid to quickly substitute itself into the RNA sequence. Once that happens, the cell’s DNA processing mechanism is severely damaged. This damaged mechanism then breaks the cell’s ability to properly and precisely weave together intricate proteins. The cell either detects this DNA damage, or just errantly due to the broken machinery, then starts generating damage alerting proteins. This action is what is called retinoid-induced apoptosis (cellular suicide). But, the damaged cell simply can’t hold its breath and kill itself off. No, it needs some help. Therefore, the damage alerting proteins are truely pleas for that help being sent out to the immune system. The immune system responds, calls in the troops and kills the now damaged and defective cell. There’s a bit more to it, but this process is what modern medicine has mistakenly termed “auto-immunity.” This fabricated term is especially wickedly evil because “auto-immunity” is just the downstream consequence of subtly overdosing on a so-called vitamin.
What may surprise you is that these exact processes were observed and documented in the vitamin-A deficiency studies conducted back in the 1920s. However, since the term autoimmunity had not been coined until the 1960s, these early researchers referred to this unexplained phenomenon as the immune system’s foreign body response being activated when there was clearly no foreign body (bacteria or virus) present. These early researchers thought they were observing some mysterious immune response due to vitamin-A deficiency. But, they also clearly knew that the immune response was a follow-on reaction to the apparently already self-destructing tissue. These researchers were also quite certain that the immune response did not initiate the tissue damage. They were also very certain it was not due to infection. However, what they did not know, was that their experiments were not inducing vitamin-A deficiency at all.
Now, let’s get to know the vitamin-A and retinoic acid villains a little bit better. From the National Institute of Health:
Source: http://livertox.nih.gov/VitaminARetinoids.htm
Background:
Vitamin-A is a retinoid and a fat-soluble vitamin that is commonly found in eggs, milk and liver and in the form of provitamin-A in carotenoids in fresh fruits and vegetables particularly those with red, orange or yellow color. … and (cod liver oil)
Hepatotoxicity:
Normal doses of vitamin-A are not associated with liver injury or liver test abnormalities, but higher doses (generally more than 40,000 IU daily, ~12,000 μg) can be toxic. Acute toxicity is caused by a single or a few repeated very high doses (generally >100 times the RDA arising within days to weeks with a typical symptom complex of severe headache, nausea, vertigo, blurred vision, muscle aches and lack of coordination, followed by skin desquamation and alopecia.
…
Chronic hypervitaminosis A usually arises 3 months to many years after starting moderately high levels of vitamin-A (generally 10 times the RDA) and is marked by dry skin, cheilosis, gingivitis, muscle and joint pains, fatigue, mental dullness, depression and liver test abnormalities.
Mechanism of Injury:
Vitamin-A in high doses is a direct toxin. Excess vitamin-A is stored in stellate cells in the liver and accumulation can lead to their activation and hypertrophy, excess collagen production, fibrosis and liver injury. The toxicity is dose-related and can be reproduced in animal models.
2 http://ajcn.nutrition.org/content/83/2/191.long
3 Image source: https://commons.wikimedia.org/wiki/File:Pre-mRNA-1ysv-tubes.png
There have been many experiments proving vitamin-A toxicity in animals. Here are a few that particularly stand out for me. Firstly, is “The action of vitamin K in hypervitaminosis A.”4 study from 1947. By S. E. WALKER, E. EYLENBURG AND T. MOORE. Dunn Nutritional Laboratory, University of Cambridge and Medical Research Council
Thus, by 1947 the toxicity of vitamin-A overdose had been very well established, and the authors of the above report are looking for potential antidotes to it. What they document is not only that do their lab animals quickly develop lesions and hemorrhages due to the excess vitamin-A they are fed, many of them suffer spontaneous bone fractures too. The vitamin-A toxicity action, and it occurs almost unbelievably quickly, depleted the calcium from the bones of the animals. So incredibly severe is this condition that the researchers report they were inadvertently breaking the bones just trying to handle the rats.
As already stated the most characteristic lesions in with hypervitaminosis A appear to be hemorrhages,
variable in intensity and distribution, and also spontaneous skeletal fractures, which occur mainly in young rats. Both these injuries were produced in various groups in the present experiments, and the apparent effect of age was confirmed. Thus, at autopsy the hemorrhages found in adolescent were more widespread and severe than those in young rats, but spontaneous fractures were absent.
I like this statement from their abstract: “rats were fed on massive doses of vitamin-A for periods varying from 10 to 18 days.” Then in the Experimental Details section of the report, they define exactly what “massive” means: it is “one drop of halibut-liver oil per rat per week.” Therefore, for these rats that’s a whole three or four drops of halibut-liver oil in their entire lifetime. That’s all that was needed to induce serious disease and bone fractures. Very similarly from an earlier study from 1937 we have:
The rats were fed 0.5 cc. daily, or a dosage of 20,000 units of vitamin A. The outstanding features of the disease produced in about 10 days were failure to grow, inflammatory changes in the eyes with exophthalmos and changes in the bones resulting in spontaneous fractures.
Quite amazingly, where we have a vitamin-A toxicity experiment producing the de facto primary vitamin-A deficiency condition of xerophthalmia! Astonishingly, it does so in just 10 days too.
An additional study I want to reference is:
The Effects of Vitamin-A and Citral on Epithelial Differentiation in vitro 1.
The Chick Tracheal Epithelium
by MARGARET B. AYDELOTTE
J. Embryol. exp. Morph., Vol. 11, Part 1, pp. 279-291, March 1963
Naturally, vitamin-A toxicity has also been proven many times in vitro (“in glass”). However, what makes this research so interesting is the effects of exposing various epithelial tissue types to high levels of vitamin-A in vitro.
Though vitamin-A deficiency appears to have relatively little effect on skin and other epithelia that are normally keratinized, these epithelia change with high concentrations of vitamin-A. When the vitamin was applied locally to the skin of rats (Sabella, Bern & Kahn, 1951) or administered orally in very large doses (Studer & Frey, 1949), the skin failed to keratinize normally, while the immature, non-keratinized cells proliferated rapidly and formed a thick epithelium.
The reason this report is important to us is that what we want to understand better is the effect vitamin-A has on the stem cells of these epithelial tissues. Firstly, I just want to highlight this report’s reference to earlier research done by Fell & Mellanby, in 1953; and Fell in 1957. Therefore, by 1953 the researchers were getting a pretty good understanding of the profound effect vitamin-A had on epithelial stem cells and the thought to be differentiation process.
High concentrations of vitamin-A also influenced epidermal differentiation in vitro: when embryonic chick skin grown by the organ culture method was treated with relatively high concentrations of vitamin-A, normal keratinization was inhibited and a mucus-secreting, sometimes ciliated epithelium, remarkably similar to that of the normal nasal mucosa, developed instead (Fell & Mellanby, 1953; Fell, 1957).
From these results it is clear that vitamin-A exerts considerable influence over epithelial differentiation: excess inhibits keratinization of epithelia and some-times induces mucous metaplasia, whereas deficiency in vivo inhibits mucus secretion and causes keratinization of many mucous membranes.
And then in the discussion section of the report, we have:
Although vitamin-A is essential for the normal maintenance of mucus secretory epithelia, and in high concentrations it can promote mucous metaplasia of some keratinizing epithelia, in the experiments just described high concentrations of vitamin-A actually inhibited synthesis and secretion of mucus by the chick tracheal epithelium. Previous experiments, however, show that the concentration of vitamin-A need not be abnormally high to inhibit mucus secretion by the tracheal epithelium; indeed, in young chicks, secretion is partly inhibited by the normal concentration of vitamin-A in the body (Aydelotte, unpublished).
Overall, this is an excellent study and report. But, as you dig into it you’ll see some rather confusing and apparently contradictory statements regarding similar effects induced by vitamin-A deficiency. However, once you understand what really happened in the vitamin-A deficiency experiments, you’ll understand why the author makes these statements. Additionally, when the author states that elevated vitamin-A levels: “induces mucous metaplasia” I believe what she was really witnessing was not mucus, rather it was leaking lymph fluids.
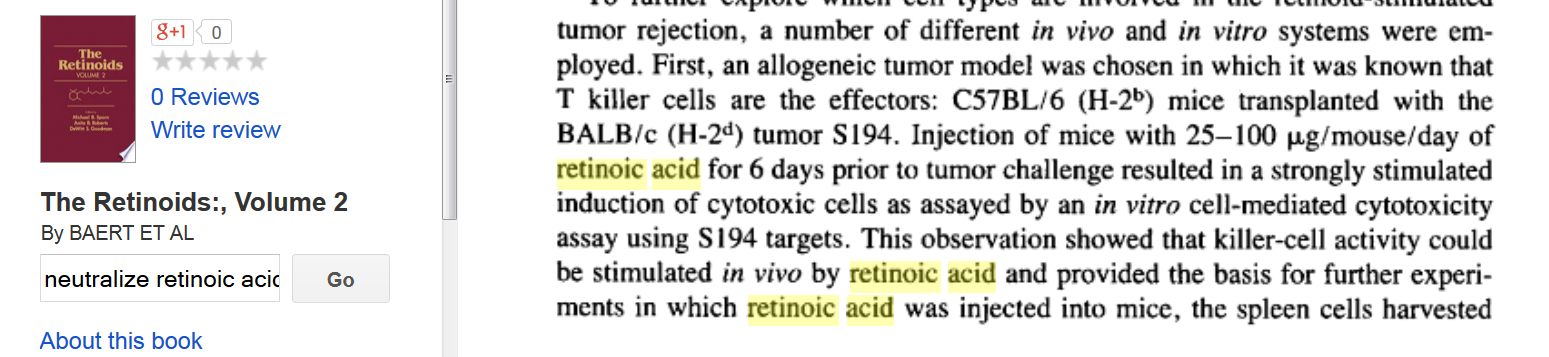
Figure 2 Killer-cell activity stimulated into action with retinoic acid
Source: The Retinoids:, Volume 2 By BAERT et al., page 383 |
Now, since this report documents the in vitro tissue response to elevated levels of vitamin-A we don’t get the benefit of seeing what the immune system’s follow-on responses and actions are to that tissue destruction. But, no worries, there are other reports that document it. At right is just one example.
There are many other research papers and hundreds of experiments reporting exactly the same effect. Unbound retinol, and retinoic acid absolutely do cause cells to initiate immune assisted apoptosis. Therefore, there can be no doubt that both retinol, and retinoic acids are toxins.
Next, let’s have a look at a partial list of documented side direct effects due to short and medium-term exposure to retinoic acid (as a medical treatment).
In my previous e-book, I wrote quite extensively about the use of retinoic acid being used to treat acne. I’ll summarize some of that information here. The most popular brand name used was Accutane. However, there are other brand names, and many generic versions of it too. The use of the drug is really a deal with the devil. It offers short-term gains in exchange for a potential lifetime of long-term pain and suffering. The government regulatory agencies are very well aware of the horror show this “drug” is inflicting upon our youth (tens of thousands of them), so they have put in some more restrictive guidelines, and produced some nice brochures. Of course, they have not pulled the drug off the market. Naturally, many doctors ignore these more restrictive guidelines and are still prescribing the “drug” for even mild cases of acne. The more common side effects are: (from the iPledge program page)
problems with the skin, pancreas liver, stomach, bones, muscles, hearing, vision, lipids, allergic reactions, blood sugar, or red and white blood cells. The most common, less serious adverse events include dry skin, chapped lips, dry eyes, and dry nose that may lead to nosebleeds.
Do you recognize these side effects? Yes, they are the symptoms of vitamin-A poisoning. But, wait, there are even more side effects, including fatigue, trouble sleeping, trouble concentrating. And, there are still even more serious side effects listed for this drug:
Depression
Psychosis (seeing or hearing things that are not real)
Suicide Some patients taking isotretinoin have had thoughts about hurting themselves or putting an end to their own lives (suicidal thoughts). Some people tried to end their own lives and some people have ended their own lives.
and
Patients on isotretinoin have been known to become depressed or to develop other serious mental health problems. Some people have had thoughts of hurting themselves or putting an end to their own lives. Some people tried to end their own lives and some have ended their own lives. There have been reports that people on isotretinoin were aggressive or violent.
That’s right, suicide is documented as just a side effect of taking this so-called acne medication. Are doctors really giving an extremely toxic and powerful chemotherapy drug to trusting teenagers for acne? You bet they are. And this wonder drug has been a huge seller.
One of the most shocking reported side effects of this wonder drug is reduced IQ, and even permanent brain damage. But, the medical establishment doesn’t seem to be too concerned about that little detail either, because they have more drugs to sell you for that new condition of reduced IQ.
The most immediate risk of using Accutane is that to the unborn child. Therefore, all women who could potentially become pregnant are asked to enter into the “iPLEDGE”5 program and contract, and are supposed to be closely monitored by their prescribing physician.
From the iPledge program Patient Introductory Brochure:6
There is an extremely high risk that severe birth defects will result if pregnancy occurs while taking isotretinoin in any amount, even for a short period of time.
What are the risks exactly?
Birth defects which have been documented following isotretinoin exposure include abnormalities of the face, eyes, ears, skull, central nervous system, cardiovascular system, and thymus and parathyroid glands. Cases of IQ scores less than 85 with or without other abnormalities have been reported. There is an increased risk of spontaneous abortion, and premature births have been reported.
Documented external abnormalities include: skull abnormality; ear abnormalities (including anotia, micropinna, small or absent external auditory canals); eye abnormalities (including microphthalmia); facial dysmorphia; cleft palate. Documented internal abnormalities include: CNS abnormalities (including cerebral abnormalities, cerebellar malformation, hydrocephalus, microcephaly, cranial nerve deficit); cardiovascular abnormalities; thymus gland abnormality; parathyroid hormone deficiency. In some cases death has occurred with certain of the abnormalities previously noted.
Wow! All that sounds awfully bad. So, what happens if a woman does become pregnant? Although it is not explicitly stated in the iPLEDGE brochure, other medical websites state it clearly: “Because the answer to a pregnancy [on isotretinoin] is a termination.”
Just how toxic is Accutane? Well over the full course of treatment for young adults the total amount of the drug taken is about 5 or 6 grams. If that amount were taken in one shot, it could easily be a lethal dose. What the drug makers want you to believe is that the functional mechanism of retinoic acid is in reducing the size of the sebaceous glands via some magical “sebosuppressive” effect.7 But, that’s not the truth. The real true mechanism is that it is poisoning and killing the stem cells that reside in the sebaceous glands, and elsewhere. If the process goes a little too far, it will destroy the functioning of the sebaceous glands altogether. Of course, if the stem cell kill-off was limited to just the sebaceous glands of the skin it might not be too horrible. But, it’s not. It kills stem cells all over the body.
Here’s just a partial list of the conditions most commonly being reported by people who have been adversely affected by Accutane, et al.
Arthritis, diabetes, migraines, pain disorders, intracranial hypertension, cheilitis, eczema, chronic dry eyes, glaucoma, acquired food sensitivities, acquired food allergies, acquired seasonal allergies, Inflammatory Bowel Disease, Colitis, Irritable Bowel Syndrome, Post-Chemotherapy Cognitive Impairment, Anhedonia, depression, anxiety, seizure disorders, Depersonalization Disorder, ADHD, Chronic Fatigue Syndrome, erectile dysfunction, reduced libido, reduced testosterone levels, hair loss, chronic dry skin, increased scarring of skin, weight loss, heat intolerance, raised liver enzymes, thyroid abnormalities, decreased ability to build muscle, and more.
In addition to the erectile dysfunction, reduced libido, reduced testosterone levels reported here, we’ll soon get a much better understanding why this wonder drug could have a devastating effect on longer term fertility too.
If you are wondering just exactly how does retinoic acid toxicity cause a disease such as diabetes, here it is in a nutshell. It causes the blockage and eventual disintegration of the ducts of the pancreas.
5 https://www.ipledgeprogram.com/
6 https://www.ipledgeprogram.com/Documents/Patient%20Intro%20Broch.pdf
7 Oral 9-cis-retinoic acid versus 13-cis-retinoic acid in acne therapy.
The use of retinoic acid as an acne treatment originated from the use of it in chemotherapy. This is not just approximately the same drug. No, it is exactly the same drug, the same molecule, the same isomer of it, and even the same product named version of it: Accutane. So, if the use of Accutane as an acne treatment is the medium stress test of retinoic acid toxicity on the human body, then being given the Accutane “treatment” in cancer cases is the extreme stress test. Here are some of the documented so-called side effects:
- Headache, fever, dry skin, dry mucous membranes (mouth, nose)
- Bone pain
- Nausea and vomiting
- Rash
- Fatigue
- Mouth sores
- Itching
- Sweating
- Eyesight changes
- Back pain
- Pain in muscles and joints
- Allergic reaction
- Abdominal pain
- Poor appetite
- Dizziness
- Drowsiness
- Insomnia
- Anxiety
- Numbness and tingling of hands and feet
- Weakness
- Loss of concentration, and sleep problems
- Hair loss (thinning)
- Dry eyes, sensitivity to light
- Decreased night vision, which may persist after treatment is stopped
- Swelling of the feet or ankles
- Low blood counts
- Anemia and/or bleeding
- Abnormal blood tests: increased triglyceride, cholesterol and/or blood sugar levels.
- Increases in blood tests measuring liver function. These return to normal once treatment is discontinued (see liver problems)
- Blood clots
- Pulmonary embolus or stroke
- Pancreatitis (inflammation of the pancreas)
- Skin desquamation (peeling and shedding)
- Problems with kidneys
- Inflammation of the liver
- Inflammation of the stomach
- IBD
- Muscle problems
- Hearing loss, and ringing in the ears
- Problems with lipids
- Problems with blood sugars
- Inflamed, and peeling of the lips
- Dry nose and mouth, nosebleeds
- Depression
- Thoughts of hurting oneself, or others
- Psychosis (seeing or hearing things that are not real)
- Suicide
- Bone density loss
- And even more …
Source: http://chemocare.com/chemotherapy/drug-info/13-cis-retinoic-acid.aspx
See also: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0044974/ - DDIC601821.side_effects_section
Now that is definitely, and amazingly, the head to toe destruction of the human body. More importantly, we should all now recognize this list for what it really is. It is head to toe autoimmune diseases. How often has this “medication” been proven to cause all this destruction? Well, at least a million times over. That’s correct. Even though retinoic acid (Isotretinoin) is a really shitty, and highly ineffective chemotherapy drug,8 it has been widely used since the early 1960s. Of course, it is ridiculously ineffective. What the “drug” is doing is simply poisoning the entire body. What it is really doing is decimating the body’s stem cell population to such an extent, it appears to pause the cancer process. Naturally, for most of the few people that survive this medical torture treatment, their cancers just reappear after their stems cells start growing again. Where in the hell did this bizarre concept of attempting to poison sick people with cancer back into health even come from in the first place? You probably don’t want to know.
Even more astonishing is that there are studies that show that the use of retinoic acid in chemotherapy actually not only lowers one’s chances of survival when compared to placebo, it accelerates patients into even earlier death. Not surprisingly, it has been an enormously profitable “drug” too.
But, let’s not worry about those little poisoning for profit details for now. What we need to focus on is that retinoic acid has been used (and mostly unsuccessfully) millions of times over as a cancer treatment, and every single time it causes many of the above noted so-called side effects. And of course it has, because this is what they think they need the drug to do. Therefore, clearly, then these are not side effects. They are the direct response and results of a body-wide poisoning.
8 Mortality in the Randomized, Controlled Lung Intergroup Trial of Isotretinoin
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2881192/
The wonders of vitamin-A and retinoic acid have not been ignored by dermatologists either. Both vitamin-A and retinoic acid have been widely used in dermatology, and for over fifty years now too. These retinoids have been applied topically to the skin for its perceived skin thickening and thought to be rejuvenating properties.
To elicit a slow thickening effect, vitamin-A is used. To elicit a more rapid effect, retinoic acid has been used. The mechanism of the treatments is to induce more rapid cellular division of the stem cells of the skin. However, in both scenarios the treatment almost always eventually leads to inflamed skin and even thinner skin in the long run. Therefore, the skin thickening effect is always short lived. Additionally, in the longer term, most dermatology patients treated with the retinoids need to stop the “treatments” because the inflammation just becomes too severe, and other little complications such as skin lesions show up. That’s right, if the treatment is applied just a little too long, or at just a little too high of a concentration, the result is inflamed skin, and even hemorrhaging and lesions of the skin.
But, like the dermatologists prescribing Accutane for acne, the dermatologists here are glossing over the critically important little hidden consequences of forcing the more rapid stem cell division. That is, it is actually depleting the skin’s stem cell population at the same time. We’ll go into the reasons for why this is in a subsequent chapter.
Equally important, and what many of the dermatologists probably don’t understand, is that the stem cells are not just magically responding to the elevated levels of the retinoids. No, the stem cells are actually being poisoned. The body detects that they have been poisoned, and then tries to rapidly grow them off of the body. So, yes, the skin “thickens” for a while, but it’s temporary, and it’s definitely not a good thing. Ultimately, then the skin is left thinner and depleted of many of its important stem cells. Nice work guys.
Regarding the understanding of the real functioning of the retinoids, it appears that medical science catches on very slowly. It has taken over fifty years for dermatology to start to recognize and accept the fact that, in the long run, the retinoids are just not working out very well as skin conditioning treatments. Nonetheless, word does not travel fast. There are at least 700 everyday cosmetic products, such as creams or lotions, sunscreens, etc., that contain retinoids. Now, could this bad situation quickly get a whole lot worse? You bet it does. Just expose this retinoid loaded skin to sunlight, and you’ll vastly increase your chances of getting skin cancer. That’s more nice work guys.
Why and how does vitamin-A promote skin cancer? The condensed version of the story is that vitamin-A is an incredibly efficient light-absorbing molecule. This light absorbing property is probably one of the primary reasons it is present in nearly all plants. But, now with that same light absorbing molecule residing within the lipids and cells of our skin, it acts as little embedded microwave ovens when we go out into the sun. This embedded molecule then brings in a tremendous amount of solar radiation directly into our cells and quickly turns it into heat.
If you consume massive amounts of vitamin-A, over a short period of time, this results in what’s termed acute toxicity. People have been killed by doing it. There’s even a well-documented case of a man who was killed by overdosing just from drinking massive amounts of carrot juice. Other times, it’s from more inadvertent poisonings.
A newborn child, who mistakenly was given 0.09 mmol (25 mg) daily or 25 µmol per kilogram for 11 days died of apparent vitamin-A toxicity.
Health, Survival, and Vision
Alfred Sommer and Keith P. West
With James A. Olson and A. Catherine Ross
Oxford University Press, 1996
ISBN: 9780195088243
See: page 243
Of course, this extreme fatal vitamin-A poisoning scenario has been directly reproduced in animals.
Young monkeys, when given lethal doses by intramuscular injection, fall into a deep coma, often have convulsions and respiratory irregularities, and finally die of either respiratory failure or convulsions.
Source: Vitamin-A Deficiency; Health, Survival, and Vision, page 243
That’s right, if you get a bit too much of this so-called vitamin it can kill you. And, if it does not kill you, here’s a nice summary for the more common symptoms of its longer-term toxicity:
Signs and symptoms of Chronic Vitamin-A Toxicity:
Children: Alopecia, anorexia, bone pain and tenderness, bulging of fontanelles, craniotabes, fissuring at lip corners, hepatomegaly, hyperostosis, premature epiphyseal closure, photophobia, pruritis, pseudotumor cerebri, skin desquamation, skin erythema.
Adults: Alopecia, anemia, anorexia, ataxia, bone pain, bone abnormalities, brittle nails, cheilitis, conjunctivitis, diarrhea, diplopia, dryness of mucous membranes, dysuria, edema, elevated CSF pressure, epistaxis, exanthema, facial dermatitis, fatigue, fever, headache, hepatomegaly, hepatotoxicity, hyperostosis, insomnia, irritability, menstrual abnormalities, muscular stiffness and pain, nausea, negative nitrogen balance, nervous abnormalities, papilledema, petechiae, polydypsia, pruritis, pseudotumor cerebri, skin desquamation, skin erythema, skin rash, skin scaliness, splenomegaly, vomiting, weight loss.
Ellenhorn's Medical Toxicology: Diagnosis and Treatment of Human Poisoning. 2nd ed.
Baltimore, MD; Williams and Wilkins, 1997., p. 1021
**PEER REVIEWED**
And in the shorter timeframe, or if you are younger or smaller, it’s:
Early manifestations of hypervitaminosis A include fatigue, malaise, lethargy, irritability, psychiatric changes mimicking severe depression or schizophrenic disorder, anorexia, abdominal discomfort, nausea and vomiting, mild fever, and excessive sweating. Children may fail to gain weight normally, and adults may lose weight. Slow growth, premature epiphyseal closure, painful hyperostosis of the long bones, arthralgia, myalgia, hypercalcemia, and hypercalciuria have been reported. CNS signs and symptoms also include increased intracranial pressure, bulging fontanelles in infants, headache, papilledema, exophthalmos, vertigo, and visual disturbances. Dryness and cracking of the skin and lips, scaling, pruritus, brittle nails, alopecia, erythema, hyperpigmentation, and massive desquamation may also occur. Hypomenorrhea, hepatosplenomegaly, cirrhosis, jaundice, elevated serum AST (SGOT) and ALT (SGPT) concentrations, urinary complaints, anemia, leukopenia, leukocytosis, and thrombocytopenia have also been reported. Increased plasma concentrations of vitamin-A usually occur but do not necessarily correlate with the severity of toxicity.
Source: As above
Here’s Sommer’s shortened version of the list:
Approximately 50 signs of chronic toxicity have been reported, of which the most frequent are alopecia, ataxia, bone and muscle pain, cheiltis, conjunctivitis, headache, hepatotoxicity hyperlipemia, hyperotosis, membrane dryness, pruritus, pseudo tumor cerebri, various skin disorders and visual impairment.
Source: Vitamin-A Deficiency; Health, Survival, and Vision, page 243
Firstly, you’d think that seeing that there are over 50 signs of chronic toxicity it would have raised some serious doubts as to the claim that this is even a vitamin. But, it gets even better here. Aren’t those all the same symptoms of vitamin-A deficiency. I mean seriously, as Sommer and his co-authors were typing up this paragraph how could they have not possibly noticed that conjunctivitis, skin disorders, and visual impairment being the identical and primary symptoms to those encountered with so-called vitamin-A deficiency?
Also, in my prior e-book, I think I made a good case that the so-called “psychiatric changes mimicking severe depression or schizophrenic disorders,” are not at all just “mimicking” the severe depression or schizophrenic disorders. Rather, it’s the complete opposite. Those named conditions are being caused by vitamin-A toxicity. In other words, schizophrenia is simply caused by vitamin-A toxicity.
Vitamin-A toxicity is causing birth defects.
The teratogenic toxicity of vitamin-A is well known, and it’s very well-documented. It has been of course repeatedly proven in many animal experiments and widely recognized in humans. It was interesting for me to learn that out of the about 800 known toxins to humans only 20 of them are proven to be teratogenic. In other words, a toxin must be extremely hazardous to make it into this exclusive top 2.5% group of toxins. Amazingly, vitamin A is in that elite group, and of course retinoic acid is too and even on par with thalidomide. I’ve also devoted a considerable amount of space in my previous e-book to this topic of vitamin-A causing birth defects, so I’m not going to reiterate it all here. However, when combined with all the other information I’ve presented in this chapter, it’s rather damn clear that it is one hell of a toxic substance for us to be calling it a vitamin.
Are we sure this is Vitamin-A and not Poison-A?
With all the above, does it just not intuitively make you seriously question the claim that this is a vitamin at all? What’s your gut feel on it? What are your instincts telling you?
Now, there have been two very important points I wanted to make in this chapter. Firstly, that vitamin-A will normally, and naturally convert to retinoic acid. This is not a “theory,” and it is not speculation, it is completely proven in clinical research. Therefore, over time, we are all very slowly giving ourselves the retinoic acid “treatment.” For most adults, it is just going to ever so slowly progressively get worse as we get older.
The second, and more important, bit of information presented in this chapter is that you need to be very familiar with the description, scope, and magnitude of the tissue and organ destruction caused by retinoic acid. The reason you need this understanding is that I want you to be able to recognize these conditions again in the context of the early experiments conducted to prove the vitamin-A deficiency theory. What I am going to show you in a subsequent chapter is that the so-called vitamin-A deficiency experiments were nothing more than high dose retinoic acid experiments!
In my previous e-book, there’s a chapter on the autoimmunity flare-up process and how the stratified epithelium is the primary sites of destruction in response to vitamin-A toxicity, and especially so in the skin. If you have not yet had a chance to read that chapter, I believe that it is worth your time. I present a lengthy and logical explanation for the sequence of events involved. I explain how the inflamed and damaged cells lead to the supposed “auto-immune” response. I go over why the immune system is not at all defective in attacking the affected cells of the various epitheliums. Now, here in this chapter, we are going to add some more information and explanations as to why the epithelium is such an important tissue structure to fully understand and appreciate in the context of the chronic diseases.
I think one of the hardest aspects of my overall theory to accept is the claim that all the auto-immune diseases are fundamentally one and the same condition. I make the claim that the organ the named autoimmune disease most prominently presents in is a red herring, and is almost meaningless in regards to the etiology. Conversely, what’s extremely important is that the named disease presents itself in the epithelium of the organ. Therefore, the auto-immune diseases are all diseases of epithelium, and / or the consequences of the destruction of these epithelial tissues. Of course, there’s some very strong clinical evidence supporting this statement. Here’s just one example:
Much to our surprise, we found that immunologically, type I diabetes and multiple sclerosis are almost the same - in a test tube you can barely tell the two diseases apart," said Dr. Dosch, the study's principal investigator, a senior scientist in the HSC Research Institute, and a professor of Pediatrics and Immunology at the University of Toronto (U of T). "We found that the autoimmunity was not specific to the organ system affected by the disease. Previously it was thought that in MS autoimmunity would develop in the central nervous system, and in diabetes it would only be found in the pancreas. We found that both tissues are targeted in each disease.
ScienceDaily, 22 March 2001.
http://www.sciencedaily.com/releases/2001/03/010322074643.htm
In both MS and in diabetes, the immune system is responding to the apparently misbehaving stem cells of the epithelial tissues. In the disease labeled Multiple Sclerosis, it just happens most aggressively in the epithelial tissues comprising the myelin sheaths wrapping nerves, and in the other disease labeled Diabetes, it just happens most aggressively in the epithelial tissues comprising ducts of the pancreas. However, the named organ is almost meaningless in understanding the real mechanism of the disease. The root mechanism of the disease is the destruction of the epithelial tissues within the organ. What so important about the epithelial tissues is that it is a fundamental tissue type that not only covers the exterior of the body, it also lines the cavities, gland ducts, blood vessels and organs throughout the body.
Now, if you’ve taken the time to read the reported details from the vitamin-A deficiency/toxicity experiments, regardless of the organ, what’s the primary tissue structure that’s always affected? It’s the various epithelial tissues. Therefore, it’s critically important to zoom-in and see that we are not looking at just organ destruction, rather it is the destruction of the epithelial structure within, or that makes up, the organ. From there, we then need to drill down just a little bit deeper to see that it’s the stem cells that are hosted along the basal membrane of that epithelial that are the primary source of the disease. This is because the stem cells are the primary target of vitamin-A toxicity. As the stem cells fall victim, the overall tissue slowly starts to degenerate, and ultimately disintegrates. Therefore, the disease quite literally progresses from the bottom up, or from the inside out. If this disease process happens in the epidermis, then you have eczema. If it happens in the pancreas, you have diabetes. If it happens in the lungs, you have asthma. If it happens in the reproductive tissues, then you have infertility. If it happens in the myelin sheaths surrounding the nerves, you have MS. If it happens in the eyes, you have xerophthalmia. If it happens in the nephrons of the kidneys, you have kidney disease. If it happens in the GI tract, you might have Crohn’s or colitis, and on and on. Well, you get the idea. Any organ or any epithelium can and will be affected by vitamin-A toxicity. This aspect of its toxicity is not just some “theory.” It has been absolutely and completely proven, and proven thousands of times over, in both animal experiments and with the so-called cancer treatments in humans.
Of course, in most people who experience vitamin-A toxicity (the so-called auto-immune diseases), it is usually not just one organ or tissue, that’s affected at one time. Often, it is two or three organs that are affected at the same time. But, naturally, that is just the beginning of the overall disease condition. As the various epithelial tissues of the organs begin to fail, the primary function of the organs obviously begins to fail too. From there we cascade down into the pit of disease and inflammation hell. Obviously, dealing with failing organs is damn horrific. However, the situation can, and very often does, get a whole lot worse. The disease condition will cascade throughout the body, severely affecting non-epithelial tissue such as the bones, the blood’s oxygen carrying capacity, and of course the brain too.
Naturally, with the self-destructing epithelium, in a range of organs, the tissue’s critical barrier function is also lost, leading to all kinds of chronic infections. Last, but not least, once the DNA damage stem cells are unnaturally forced off the basal membrane and into circulation, or possibly to the backside of the basal membrane, cancer is next on the agenda.
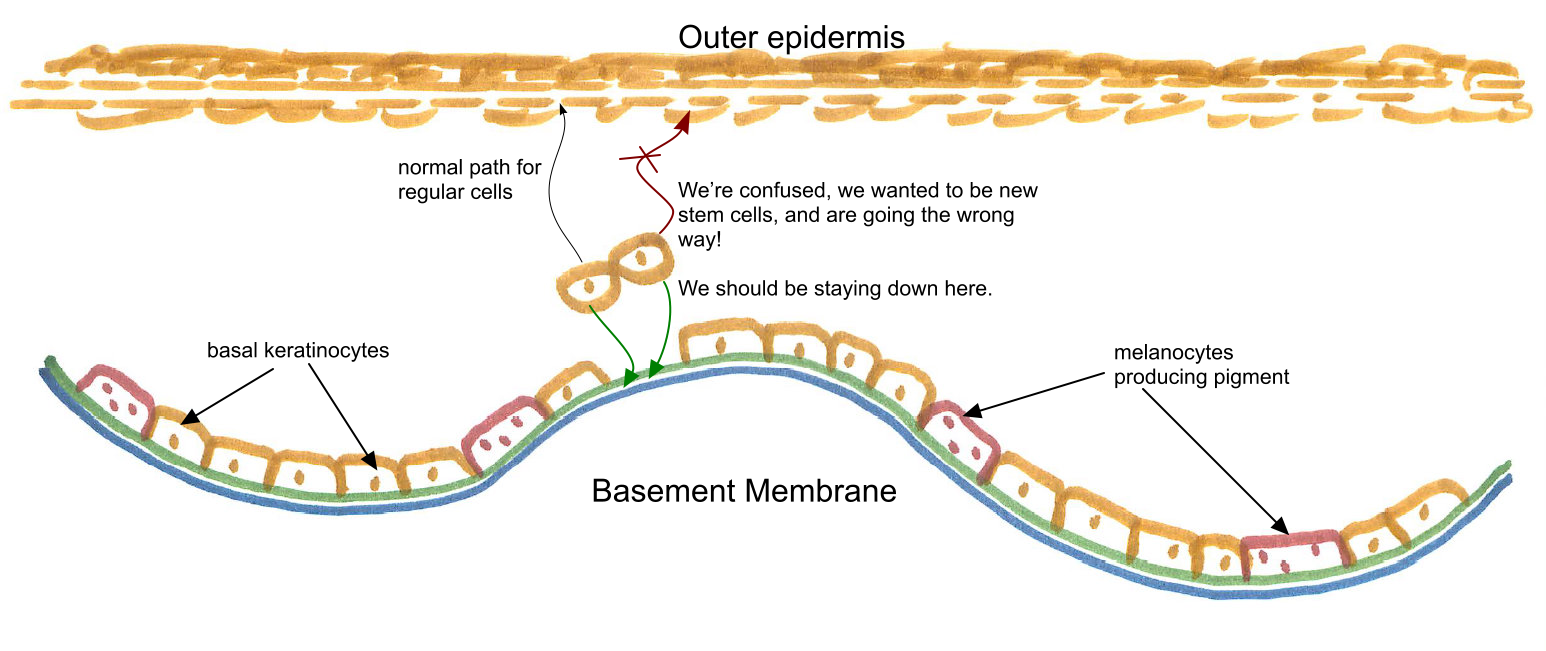
Figure 3 The basal keratinocytes driven onto the wrong path
|
Next, we now need to have a very good understanding of what the term “stem cell differentiation” means. Naturally, this is a man-made term applied to a process that stem cells undergo to maintain overall tissue structure. Within the epithelial tissues, all new cells originate from the stem cell population. The stem cells reside on, and along, a thin membrane at the base of the epithelial tissue. In the epithelial tissues, only stem cells are capable of dividing. Therefore, a healthy and properly functioning population of stem cells is critically important. For our discussion purposes here, we’ll primarily refer to the stratified epithelial tissue making up the skin.
I like to think of the basement membrane as a non-moving supply chain that continuously grows new cells to replenish the epidermis. Of course, the stem cells are very special cells in that when they divide they have a few choices as to what type of cell they want to grow up as. But, it is not a completely arbitrary choice either. That choice is tightly regulated and controlled. As cells are normally shed from the outer epidermis, hormonal messages are sent down to the stems cells to grow new replacement epidermis cells. But, a stem cell is a stem cell, not a more specialized one needed in the upper layers of the epidermis. Therefore, to accomplish the transformation feat of converting from stem cell to a more specialized one, the cell goes through differentiation. The differentiation process is not immediate. It is a slow process, and continually progresses until the cell eventually reaches the outside of the epidermis. As the cells migrate to the top of the epidermis, they continue the differentiation process and become more and more filled with keratin. Of course, this process goes on every day of our lives. If everything goes according to plan, as we shed and lose surface cells there’s always a slow-moving migration of new cells being grown up from the basement membrane to replenish them. If everything is kept in balance, we have nice smooth, moist, and beautiful skin to live in.
But, there’s just one little detail that I’ve glossed over. That is the resupply chain needs to be kept in equilibrium too. This means that the stem cells not only need to replenish the upper epidermis, but they also need to replenish themselves too. Clearly, if the differentiations were always in favor of epidermis cells, you’d quickly run out of source stem cells. Obviously, renewing the stem cells on the basal layer is just as important, and it needs to be renewed at almost precisely the same rate. Of course, this process must be closely regulated so that the skin does not become too thick, or too thin.
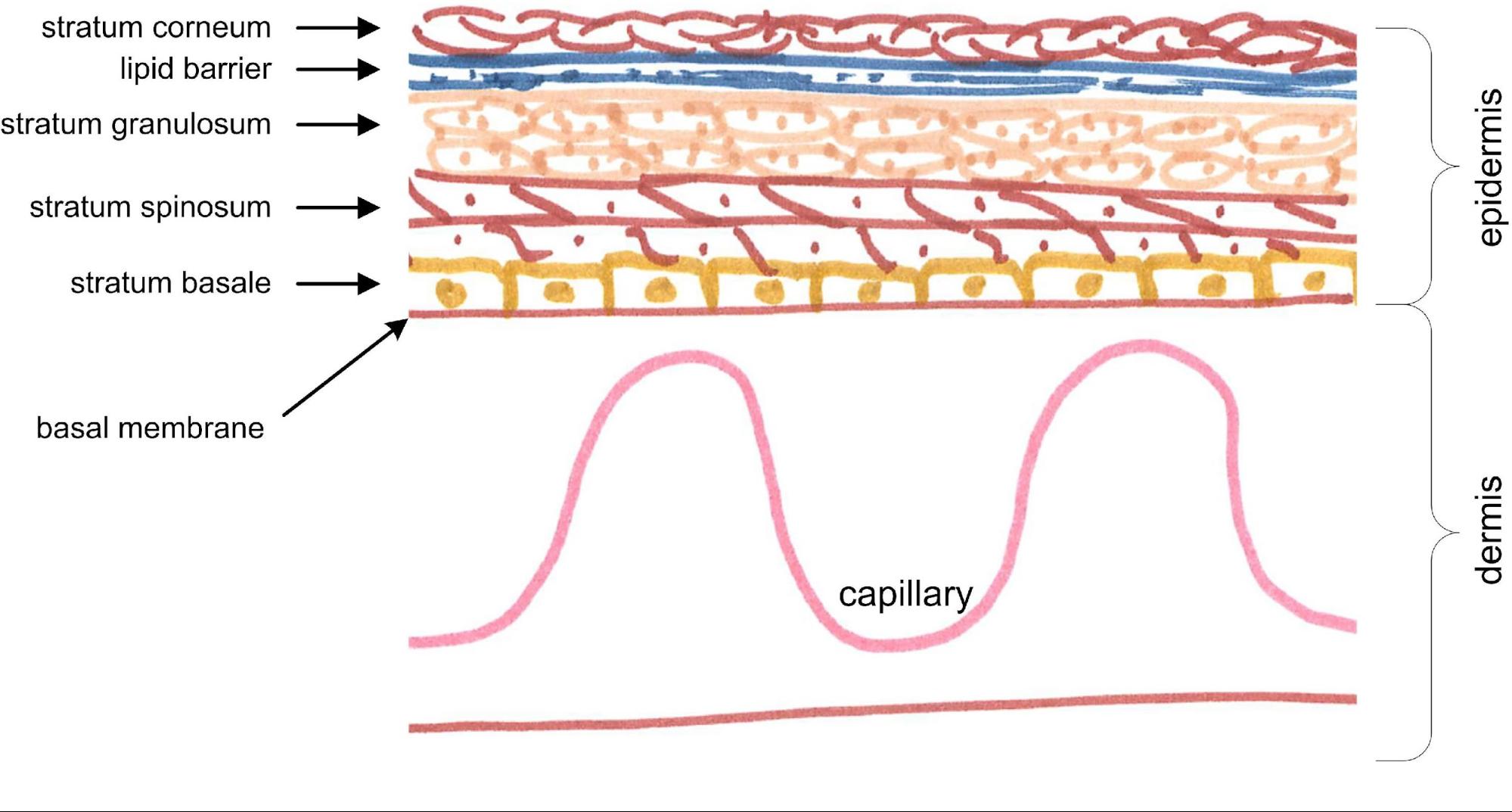
Figure 4 The stratified epithelial of the skin
Figure 5 The skin cell’s interlocking tight junctions
|
A common misconception that I’ve come across is that some people believe that when a stem cell divides, that the division of a stem cell produces one new stem cell and one new differentiating upper epidermis cell. This is not true. Once a stem cell has decided to differentiate it is committed to complete the process, and there’s no going back. Once it’s committed down one path, there’s no longer a choice. The decision was made in the RNA of the source stem cell. Therefore, both the prodigy will become what they have been programed for. So, either both the prodigy will become differentiating epidermis cells and cleave themselves from the basement membrane, or both will remain attached to the basement membrane and continue life as new stem cells.
For stem cells that have taken the differentiation decision, they start to make their slow migration out and will undergo several progressive transformations along the way. The first transformation takes place in the next layer up, termed the stratum spinosum, or the spiny layer. At this stage, the differentiating cells start growing spines. The spines serve a critical interlocking mechanism. The spines are proteins made up of cell adhesion molecules. You can think of the spines as the cells growing arms and hands so that they can grab and hold on to each other very tightly, yet elastically, and interlock. Gradually, as the cells migrate higher up, this interlocking mechanism will effectively and completely stitch all the cells together with what’s termed the tight junctions.
The cells with their completed tight junction matrix form a waterproof barrier that also prevents pathogens from getting back in.
Of course, what happened in the early vitamin-A deficiency experiments were that they induced profound, and the head to toe, destruction of all the epithelium based organs. Naturally, by failing to recognize that they were truly seeing a poisoning in action, they attributed this destruction to the deficiency. Needing to better understand the mechanism, subsequent follow-up experiments confirmed that vitamin-A had a direct and powerful influence on stem cell differentiation. The results of which only served to deepen and further solidify the belief in the vitamin-A deficiency theory. It was quickly assumed that without the retinoid influence, the stem cells had failed to differentiate properly, and this was the causal mechanism underlying the tissue’s degeneration and ultimate destruction. Therefore, retinoid influence on stem cell differentiation is one of the biggest factors in why vitamin-A is defined as a being “vitamin” in the first place.
The confirmation that vitamin-A influences stem cell differentiation was made as far back as the 1930s; so, it is not a new discovery. Therefore, the belief in the vitamin-A deficiency theory is very deeply ingrained in modern medical thinking. Of course, this knowledge of vitamin-A’s profound effect on stem cells keeps it at the very top of the list of the essential vitamins. For medical science, there’s no mistaking it.
Retinoids are ubiquitous signaling molecules that influence nearly every cell type, exert profound effects on development, and complement cancer chemotherapeutic regimens. All-trans retinoic acid (RA) and other active retinoids are generated from vitamin-A (retinol), but key aspects of the signaling pathways required to produce active retinoids remain unclear. Retinoids generated by one cell type can affect nearby cells, so retinoids also function in intercellular communication. RA induces differentiation primarily by binding to RARs, transcription factors that associate with RXRs and bind RAREs in the nucleus.
Journal of Cellular Physiology. 2011;226(2):322-330.
doi:10.1002/jcp.22417.
it’s just a goddamn poisoning!
From those observations, it was like “Yey, isn’t this great, aren’t we smart, we can influence stem cell differentiation.” Except, this is not smart science, it’s bad science and ridiculously flawed logic. Just because we can do something, does not mean that we should be doing it. But, not to miss out on a business opportunity, this new-found ability to artificially influence stem cell “differentiation” has led to vitamin-A being used in all kinds of medical treatments and applications. Moreover, it was obviously extrapolated that if a bunch of vitamin-A will significantly promote faster stem cell turnover, and differentiation, then just a little bit of it must be needed for the slower natural turnover rate too (man, I am so glad these people don’t build airplanes).
Although managing the differentiation ratio of stem cells is an important balancing act, the body (in both humans and animals) has been able to manage this process very well and has been doing it very successfully for tens of millions of years now without the retinoids. However, not only has modern medicine discovered that vitamin-A can be used to influence differentiation they’ve concluded that vitamin-A is needed for the differentiation decision. In a quantum leap of scientific arrogance and folly, they’ve concluded that vitamin-A is the secret molecule needed to control differentiation.
But, medical science has completely failed to see what they were looking at here. It wasn’t that they are magically influencing stem cell “differentiation” with added vitamin-A, it is that they are poisoning the stem cells with it. Once the cell is poisoned, the cell itself, and the body attempt to grow it off as fast as possible, often eliciting the help of the immune system along the way. Clearly then, just because we can influence stem cell differentiation with vitamin-A, does not mean we should be doing it at all. Moreover, it is a rather astonishing display of scientific arrogance to think that we are going to outsmart nature in this critical and fundamental process of managing our stem cells.
I believe that I’ve presented ample amounts of evidence to make this case against the sub-theory that vitamin-A is needed for stem cell differentiation. But, if I haven’t, nature and human history have. We now have overwhelming amounts of information and evidence that makes it glaringly obvious to see that the theory is a complete load of rubbish. This fact has been proven to be the case at least 1,000,000 times over in just the P.O.W.s of the Second World War alone. It is also proven in the evolutionary history in most of the animal species on the planet, and for like the last 100 million years now too. The stratified epithelium remains completely, and perfectly, intact in times of even prolonged multi-year starvation. This is plainly visible in both the skin, and the eyes, of humans, and in animals. Therefore, nope, the theory that vitamin-A is somehow needed to control stem cell differentiation is a complete myth and ridiculous nonsense.
Okay, if vitamin-A is not needed (at all) for normal stem cell differentiation, and we know that elevated levels of vitamin-A cause the stem cells to behave in bizarre and unnatural ways, so much so that the immune system decides to attack and kill them, what do you suppose vitamin-A really is? Well, maybe we should just listen to what the body itself is telling us it is. What the body is clearly telling us is that it’s simply a goddamn poisoning. Of course, this is no minor poisoning. It can have far-reaching and devastating downstream consequences. Next, I am now going to explain the processes and mechanisms of that poisoning in more detail.
As the differentiating stem cells migrate up into the epidermis, they need to flatten out and grow interlocking spines. The interlocking spines are needed for the cells to tightly, yet elastically bond with each other. The interlocking spines are built up from what’s termed cell-adhesion molecules. A huge number of cell adhesion molecules are needed to completely fill in the gaps between all the cells of the outer epidermis. These cell adhesion molecules then form a matrix that not only binds and holds the cells together; they form the tight junctions between the cells. Overall, this combined structure of cells and their matrix then provide the structural integrity of the tissue. If everything goes according to plan and stays on the correct schedule, we have a nice and critical barrier between the outside world and the inside of the body. The barrier function not only keeps the good things, such as water, blood and lymph fluid, in, it also keeps the bad guys out. Who are the bad guys? Oh, those are the little microorganisms that would love nothing more than to feed off our internal fluids and proteins.
Except, now with exposure to elevated retinol levels, things don’t go according to plan, nor stay on schedule. Firstly, due to the stem cell’s RNA and DNA being damaged by retinoic acid, the cell’s protein and molecule assembly machinery is broken or significantly compromised. Therefore, the cell can no longer produce the proper cell adhesion molecules. Thus, as the cell grows up through to the outer epidermis, it lacks the mechanism to bind with other cells. The critical intercellular matrix, the tight junctions, are not being properly formed and maintained.

Figure 6 The shed off outer layers of the epidermis – resulting in “mush”
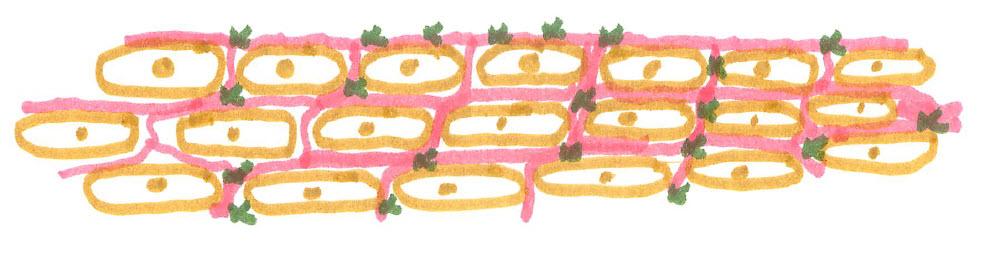
Figure 7 The destroyed epidermis – leading to infections
|
Moreover, the migrating cells do not even have the time needed to build the required cell adhesion molecules. They are simply growing way too fast. This then leads to improperly forming replacement tissues, what’s termed metaplasia. In the early stages, the tissue appears to become a bit granular and almost crystalized. Next, it progresses to where the cells become less and less bonded together with each other, and the skin quickly starts to lose its overall structural integrity. Then it progresses to where the tight junctions are malformed, broken down, and ultimately non-existent. At this stage, you pretty much just have independent cells swimming in lymph fluid. This floating cell condition is what I’ve very scientifically and accurately described as a “mush”, and it is the same condition seen in the “melting” of the cornea of the eyes.
You might be wondering how I know this process so well? I’ve watched it happen, in real-time, under my microscope, on my fingers and on the backs of my hands too. I’ve spent probably at least a hundred hours looking down through my microscope watching this process taking place. Of course, with the lost tight junction matrix resulting in the cellular mush, the lymph fluid comes leaking out. Not only is it leaking out, the top layers of flattened out and keratin filled protective cells are now nonexistent too. Shown above (Figure 6) is a bit of a close-up photo with this condition on my fingers.
With the abnormally fast growth rate from the bottom up, more exterior surface cells will be forced to flake off. But, with the stratum spinosum, and granulosum layers being malformed, they fail to maintain adequate spines and adhesion molecules to bind with the outer surface layers. These outer layers then slough off, sometimes with entire regions of surface tissue cells being lost. Subsequently, the skin in these regions then simply leaks lymph fluid. This condition is definitely not to be confused with the cells now producing mucus. Nope, it’s not mucus, rather it’s the nice sticky new home for all kinds of bacteria and viruses to nestle into.
Although much of the discussion above has been regarding the stem cell damage in the skin, and eyes, the damage is in no way limited to just those organs. The damaging effects are going on in the pancreas to cause diabetes too.
Type 1 and type 2 diabetes are characterized by progressive β-cell failure. Apoptosis is probably the main form of β-cell death in both forms of the disease. It has been suggested that the mechanisms leading to nutrient- and cytokine-induced β-cell death in type 2 and type 1 diabetes, respectively, share the activation of a final common pathway involving interleukin (IL)-1β, nuclear factor (NF)-κB, and Fas.
Source: Diabetes - Mechanisms of Pancreatic β-Cell Death in Type 1 and Type 2 Diabetes - American Diabetes Association
Up next, chronic infections. There’s no getting around it. With the skin’s barrier function is lost, the body’s outer defenses to infection are nonexistent. Once this happens, then we essentially have a wide-open wound that won’t scab over, nor heal for months. Not only is it almost impossible to not get infections, but it is also incredibly difficult to heal from them too.
How do I know this? From firsthand experience, of course. And with both the left and right hands too. Topical antibiotics might be somewhat helpful, but they are almost completely pointless too. In my experience, the only way to beat the infection is to have the skin reform its structural integrity. However, this is incredibly difficult to achieve. Not only is it a failing pile of mush, inflamed and infected, the immune system starts attacking it too. It’s a total horror show of microbiology chaos. Of course, what I’ve just described is not limited to the body’s external skin, the epidermis. No sir, it can, and is going to happen to any epithelium that goes through this self-destruction process. Infections are just inevitable. In my experience, the only real cure for them is to stop fueling the process with more {tip content="Of, relating to, or producing a toxic effect on cells."}cytotoxic{/tip} vitamin-A and let the tissue rebuild itself. Only then can the immune system finally accomplish its real job of clearing the infection. And no amount of vaccinations is going to magically protect you from the infections either. The very last thing you need is for your immune system to be chasing down more phantom infections. Naturally, the very best way to treat infections is not to get them at all. The very best way to not get infections is to have epithelium tissues that have strong and integral barrier functions.
Want infections? Just boost up your vitamin-A consumption.
In our animals, the first symptoms of a (thought-to-be) dietary deficiency, namely, failure to gain on the low fat soluble A diets, were often accompanied by certain well-defined symptoms — loss of appetite, snuffles and subsequently labored breathing. These conditions confronted us so often that we questioned whether they were the result of the dietary deficiency per se, or were due to an infection in an undernourished animal. It is perhaps significant that, in a colony of between 400 and 500 animals, those on the low fat-soluble A diets are the only ones that ever manifest such symptoms.
AMY L. DANIELS, Ph.D. AND MARGARET E. ARMSTRONG, M.D.
WITH THE COOPERATION OF MARY K. HUTTON, B.S.
IOWA CITY 1923
Naturally, the statement made above “those on the low fat-soluble A diets are the only ones that ever manifest such symptoms” probably appears very contradicting to what I’ve claimed. However, it is critically important to know that their “low fat-soluble A diets” used in these experiments were simply “high dose retinoic acid diets” in disguise.
Now if you’ve newly acquired an autoimmune disease, and are thinking of getting up to date on your vaccinations, be very careful. Your immune system is already hypervigilant, and adding the cytotoxic agents present in vaccines into the system could be like adding gasoline to a fire. Moreover, there’s very little a vaccination can do to help in this situation. Your immune system is going to have lots, and lots of time needed to build antibodies on its own to any new invaders. It also does not need to be tricked into building needless antibodies to food proteins that are now leaking into the serum from the gut.
What we need to remember, is that the epithelial structure is not present in just the epidermis. This is just a fundamental tissue structure making up much of the human body. Many other internal tissues are similar, but specialized, forms of epithelium. This include the ducts of the glands and organs. As proven in vitamin-A toxicity (and the botch deficiency) studies from the 1920s, ’40s etc. some of the most commonly affected, and the earliest affected epithelium tissues are the tear ducts, the ducts in the meibomian glands of the eye, the ducts of the pancreas, and the kidneys, and both the male and female reproductive organs.
Unlike the epidermis, the outer surface of the epithelium making up the ducts does not face the outside world. Rather, it faces the interior portal, or channel, of the duct itself. Therefore, as these interior epithelia become malformed, the rapidly growing off surface cells can’t just slough off to the outside world either. What happens is that they slough off and start plugging up the duct (tube if you prefer) too. Additionally, as the duct forming epithelium become inflamed, and swollen, the channel of the duct becomes more and more restricted, and may ultimately become completely blocked. If you’ve not read the reports from the 1920s, one other organ they reported being hugely filled with sloughing off epithelium cells, from its interior, is the bladder.
Most people are aware the autoimmune diseases go through periods of waxing and waning. But, hidden from sight, a more devastating situation is slowly and progressively developing. It’s the depletion of the stem cell populations. With excessive retinoids in circulation, and in the intercellular spaces, it is artificially influencing stem cell “differentiation” in one direction. The “differentiation” process is not just thrown off balance; it is vastly sped up too.
As the regular cells of the upper tissue layers are being destroyed, they are naturally emitting growth hormones to signal the stem cells to replicate faster. In the normal situation, the stem cells would be differentiating in a more controlled and rational manner. Normally, they’d need to differentiate at a ratio that maintains both the stem cell population, as well as resupply the upper tissue. But, by artificially influencing the “differentiation” decision in one direction they are far too often dividing to produce two upper tissue cells for every stem cell division. Therefore, the rapid cell division is producing and migrating an abnormal ratio of cells to the tissue’s outer surface, and depleting the basal layer of its source stem cells at the same time. Thus, over time we are slowly destroying the basal layer of the epithelium by using up our stem cells. Once we’ve sufficiently depleted the stem cell population, the tissue atrophies, and ultimately fails completely because it’s supply of new cells no longer exists.
In both the so-called deficiency, and toxicity studies from the 1920s, ’30s, etc. the researchers were aware of follow-on immune response to the cellular destruction. In a few of the 1922-1925 studies, they referred to this as witnessing the immune system’s foreign body response being activated. In one particular study, they were especially careful to make sure the animals did not develop infections. They kept the cages immaculately clean and hosted just one animal per cage. They were, of course, trying to isolate just one factor as causing the disease conditions. Therefore, they not only wanted to rule out infections as being the cause of disease but to also eliminate their effects on the progression and amplification of the diseases. Nonetheless, it was clear to them that the immune system was sometimes responding to the cellular destruction as though an infection were present.
Except, what they were really witnessing were early cases of induced autoimmunity. As the cytotoxin damages the cell’s RNA, the subsequent defectively constructed proteins start presenting on the cell’s surface membrane and are also being ejected off it. This strange new, and apparently foreign protein, then alerts the immune system to the cell’s malfunctioning behavior. To the immune system, the detection of strange new proteins and related cellular damage can only mean one thing; there’s pathogens present. But, unbeknownst to the immune system, it’s only a phantom pathogen. Its true identity is a cytotoxic molecule, and the artifacts produced by its damaging effects then masquerade as those of a pathogen.
I’ve detailed this process a lot more in my previous e-book. However, I just want to add a bit more to it here. Of course, the immune system then attacks the cell that’s emitting the strange proteins and hopefully kills it. If it involves just a few cells, it’s no big deal. However, as the process continues, the adaptive immune response starts to be activated. The macrophages start dragging off some of the broken cell fragments, with the damage association molecules stuck on it, into the lymph nodes. Within the lymph nodes, the immune’s beta cells use these fragments and their strange new proteins as templates to start building matching antibodies.
Other tissue cells that now present the same damage association molecules are then targeted for immediate attack. This targeting is the completely normal, expected, and required behavior by the immune system to effectively fight off pathogen infections. However, in this scenario, the damage association molecules are not generated in response to a pathogen’s damage, rather it is to a toxin’s damage. The lymph nodes will get so jamb packed with broken cell fragments they will become hugely swollen too.
Next, the killer T cells with their newly minted anti-body weaponry go on the hunt for the suspected pathogen. Of course, there is no pathogen to be found; it simply does not exist. Therefore, the immune system is never going to find it. Yet, mysteriously, more, and more of the damage association molecules keep on showing up. This is a strange new situation that effectively perplexes the immune system. The immune system can only respond more and more aggressively and keeps actively searching for the phantom pathogen. Since an apparently invading pathogen has been detected, the immune system is going to respond by sending more troops into the battlefield too. This response requires more, and more immune cells to be built. Additionally, the immune system is not interested in taking prisoners in this battle. No, whatever is going on, the immune system regards it as an existential threat that needs to be dealt with harshly and as quickly as possible. The immune system is smart, and it knows it does not necessarily need to find the actual pathogen, it may only need to find the cells that are harboring them. So, it now directly attacks any cell that’s foolish enough to present the same damage association molecules on the exterior of their cellular membrane. Of course, many other cells similarly affected by vitamin-A overload will be doing exactly that. You now have auto-immunity. However, things are not nice and tidy on this microbiology battlefield. As toxified cells are being damaged, killed off and otherwise breaking apart, fragments of those cells float away in the serum. Those fragments carry with them the new antibody targeted damage association molecules. If these fragments happen to stick on to other cells, the immune system is going to take no chances, and kill those completely innocent cells too. Let’s be very clear about this; the immune system is in no way defective in this battle. It is not confused or in some state of disorder. Rather, it is working perfectly and is heroically doing a very thorough job. The immune system is forever vigilant, and it is never going to give up the fight. Auto-immunity is auto-poisoning.
Now the process underlying autoimmunity that I have just described here should sound very familiar. What do we normally call DNA damaged, fast-replicating cells, and seemingly out of control collateral tissue growth and damage? Doesn’t that sound a lot like cancer? It’s similar enough that many people do refer to the autoimmune diseases as being non-lethal cancers. Not surprisingly, many people with autoimmune diseases do indeed have cancers at the same time too. However, the autoimmune diseases are not cancer. The crucial detail with autoimmunity is that the immune system is able to identify the damaged stem cells quick enough and efficiently to kill them off. The fight between the immune system and poisoned and misbehaving stem cells can go on for decades. The end stage is reached only when we’ve so completely depleted the stem cell population that the tissue structure fails, and thus the organ containing that tissue structure fails. Therefore, if we can maintain a healthy immune response, our autoimmune disease may just slowly kill us before we ever develop cancer.
However, there are scenarios where that’s not going to happen. As I’ve described before, once the DNA damaged stem cells (the entire cell, not fragments thereof) separate off from the basal membrane rather than properly migrating to the outer epidermis, they find their way into circulation. From there they may become attached to some other organ’s tissue, and start replicating within it. To the stem cell, it’s normal job is to diligently replicate on schedule. It’s perfectly normal behavior because when it’s natively hosted in the epithelial tissues, this is the source of all the new cells that are needed to maintain the tissue’s structure. However, now wrongly hosted elsewhere, we have a tumor developing. Exactly how many errant stem cells would be needed to start this tumor? Just one.
Naturally, if we have a healthy immune response, this errant cell may have been identified early and appropriately killed off. So, what do the experts prescribe us for treating our autoimmune diseases? Well, most commonly, it’s the steroids. The steroids function by blocking the immune system from detecting the damaged cells. This action is why it is now commonly accepted that the steroids significantly increase the risk of subsequently getting cancer.
Regardless of how and why a damaged stem cell fails to be detected by the immune system, there is an additional scenario we need to consider. With highly inflamed, and highly acidic environments, eventually, there is going to be damage to the basal membrane itself. Once there is a rupture of the basal membrane, stem cells, even completely normal, and non-damaged ones will travel to the underside of it. Next, these cells can get trapped on the wrong side of the basal membrane. Since there is nothing wrong with these stem cells, and they just reproduce on schedule, and perpetually. After all, their genetically programmed role in life is to perpetually resupply the epithelial tissue with new cells. But, by being trapped on the wrong side of the basal membrane, we now have cancer in the same hosting epithelial tissue.
There’s one more connection here between cancer and distressed epithelial tissue that I’d like to discuss, and that is vascularization. Vascularization is when new small blood vessels grow into tissue. Of course, these are not blood vessels that are normally present in healthy tissue. This phenomenon is readily observed on the face of many older people who have rosacea, and very commonly on the sides of the nose. It is also very commonly seen in people’s eyes as they become ill. Now, it is critical to understand that these new capillaries and micro-vascularization are not the expansion of existing ones. Rather, these are completely new vessels. The newly grown-in capillaries and micro vascularizations are the body’s response to the demands being made by the distressed tissue. The tissue is demanding more oxygen and nutrients and sends out special signals to entice more blood vessels to be grown in. This, in itself, is rather remarkable. Here, we can witness the amazing power of the body to not only adapt in real-time to a new demand, but it is also responding by altering its physical structure. Except, to be clear, having distressed tissues needing more blood vessels to be grown into them is not a good thing to have happen. It’s a huge red flag that a disease condition is present or developing. Of course, vascularization of the distressed tissue was induced in the so-called vitamin-A deficiency experiments, and it is almost always present in xerophthalmia too. What’s happening is as the outer layers of the epithelial tissue become dried out, and inflamed, they can no longer absorb adequate amounts of oxygen from the outside world. Distress messages are sent out, and the new blood vessels are then grown-in as alternative supply routes. Although that is absolutely remarkable, there is another disease condition that exhibits this same phenomenon, and that is cancer and of course cancer tumors. Many cancer tumors will have large and completely new blood vessels grown into them to supply them with their needed oxygen and nutrients.
A question that I keep thinking about is why is there such a high degree of variability in how the autoimmune diseases present themselves in different people. After all, if we are all being very slowly poisoned by the same toxin, then one might assume many people would present the toxicity in very similar ways. For example, why do some people first present with eczema, and others first present with MS (yes, I do know that many people present with both at the same time). What I was trying to come up with was a plausible explanation for why there are such big differences. However, on the larger scale, there are indeed recognizable patterns too. When we step back and look at the entire North American population, there are major patterns to the presentation clusters. Probably the top four most prevalent named autoimmune diseases are eczema, diabetes, asthma, and dry eyes. What’s rather astonishing, this is a very close-fit to the earliest presentation clustering seen in the rats of the early deficiency/toxicity studies done in the 1920s. What’s rather remarkable about this, is that unlike our highly variable human diets, this clustering was with all the animals on pretty much the same diet, and for the same duration. Therefore, I think it is clear, that the skin, lungs, pancreatic ducts, and the tear ducts of the eyes are the most susceptible to moderate toxicity levels. However, even with their animals on the same diet, there were variations too. Therefore, there is some apparent randomness going on.
In the human experience, there are a huge number of variables that are going to factor into who, when, and where (what tissue location) the disease conditions will first manifest themselves in. Most certainly, the studies by Mori and Bloch with fats in the diets provide us with what’s probably the most critical determining dietary factor, and that is the quantity and nature of consumed fats. On the one hand, sufficient fats are needed to emulsify and safely store retinoids. On the other hand, fats included in meals with high concentrations of plant-based sources could yield much higher absorption rates. Obviously, over the long run, fats from animal sources could be the most dangerous. The hidden vitamin-A in milk casein is right up there on the list too. Of course, then there’s the variability in one’s daily dose, animal source versus plant source (~1/20th absorbed), and the consumption of other carrier proteins such as gluten, etc.
Next, we need to keep in mind that these diseases usually develop very slowly over long periods of time. The disease has been in development well before there are any noticeable symptoms present. That’s because having just a few stem cells prematurely picked off every day is not going to manifest itself as a disease condition. It’s not until there’s been enough of a depletion of the stem cell population to cause the malformation of the tissue structure that symptoms arise. Likewise, even with the immune response selectively picking off a few misbehaving cells every day is only going to cause a very slight, and therefore not a noticeable increase in background inflammation.
From there, we need to ask the more important questions as to why does one adipose tissue collect higher concentrations of retinol than do others. Once again, I think variations in fats and the specific densities of the fats would play a significant role. The next highly variable, yet critical, factor is a person’s exposure to sunlight and drying weather conditions.
| Table 2: Mean concentration of triglycerides in males and females (mg/dL) | ||||||||
| Males | Females | |||||||
| Percentile | 5‐9 yrs | 10‐14 yrs | 15‐19 yrs | 5‐9 yrs | 10‐14 yrs | 15‐19 yrs | ||
| 50th | 48 | 58 | 68 | 57 | 68 | 64 | ||
| 75th | 58 | 74 | 88 | 74 | 85 | 85 | ||
| 90th | 70 | 94 | 125 | 103 | 104 | 112 | ||
| 95th | 85 | 111 | 143 | 120 | 120 | 126 | ||
|
Source: Lipid and lipoprotein distributions in white children ages 6-19 yr.
The Lipid Research Clinics Program Prevalence Study. Tamir I, Heiss G, Glueck CJ, Christensen B, Kwiterovich P, Rifkind BM. PMID: 7451637 |
||||||||
One of the most important observations that threads its way through all this research is that boys are more susceptible than girls. I believe we can explain this phenomenon. It’s because young girls naturally have higher serum lipid levels than do young boys.
Therefore, with these higher lipid levels, girls are better able to emulsify the dietary retinoids that enter into serum, and thus allows it to be more readily and safely stored. So, in their younger years’ girls are more protected.
However, when we get to the teenage years the parameters going into the equation change a bit, and the ratio inverts. Additionally, it is well documented that zinc is an important mineral in protecting against retinoic-acid-induced cellular damage. Men naturally use up more zinc than do women, and over the long-term, they will have more quickly depleted their zinc levels. So now, it gets tricky. Over their lifetime, women due to their higher cholesterol levels will have accumulated more retinoids within their adipose tissues. Therefore, they will generally be more susceptible to the disease conditions, yet present the diseases more gradually. Whereas, in men, after they’ve reached a storage saturation point, they are less able to mount this subtle defense and will have a more acute response to high retinoid intakes. You can think of this response as being like the mechanism that causes pH levels to make the rapid, and non-linear, changes as seen in titration experiments.
In this chapter, we are going to review and analyze the experiments that are thought to have “proven” the grand vitamin-A deficiency theory. Therefore, this is one of the most important chapters in this e-book. Please don’t just skim over it.
Before we dive into the details of why and how these experiments were truly botched we need to cover off on some long-held beliefs and concepts around vitamin-A deficiency.
Today, most people, and even the experts in ophthalmology, generally believe that vitamin-A deficiency most predominantly affects the health of the eyes and vision. But, nothing could be further from the truth. What the early vitamin-A deficiency experiments proved was the absolutely devastating head to toe tissue destruction of the entire body. The scope and magnitude of the so-call deficiency that was proven in the early experiments is nothing short of astonishing. Here’s just a brief high-level summary (in no particular order):
|
|
That’s right. That long list is much closer to the real scope and magnitude of the disease conditions reported due to the so-called deficiency. Some additional comments are noteworthy here; younger rats are significantly more susceptible than older ones. Males are more susceptible than females. Hopefully, you are spotting the pattern here. Hopefully, you are also spotting the most common named human chronic diseases in this list too; such as eczema, asthma, diabetes, arthritis, lupus, kidney disease, MS, and Sjögren’s.
This observation about the astonishing scope of the supposed vitamin-A deficiency affecting far more than just the eyes, and affecting other organs far more seriously, is made in the introductory comments by Wolbach and Howe in their 1925 study:
TISSUE CHANGES FOLLOWING DEPRIVATION OF FATSOLUBLE A VITAMIN.
From the Department of Pathology, Harvard University Medical School, and the Forsyth Dental Infirmary, Boston.
Received for publication, September 4, 1925
A number of workers have assumed that the eye and its glands alone deserved study – organs which we have found to exhibit much less striking lesions than the respiratory and genitourinary tracts and certain glands. In light of the pathology described in this paper it is no longer tenable to characterize the condition of fat soluble A deficiency by names referring to the eye pathology; i.e., xerophthalmia–keratomalacia. Atrophy of many glands, arrest of growth, emaciation, and replacement of many different epithelia by stratified keratinizing epithelium actually characterize fat-soluble A avitaminosis. The specific pathology is the widespread keratinization.
The glaring problem here with this long list of disease conditions is, how could any reasonable thinking person believe that scope of destruction could even be possibly caused by a mere deficiency? The other major problem here is that all of this destruction happened in an amazingly short period of time.
If that long list of disease and tissue destruction did not cause them to pause and deeply, and very seriously question their deficiency concept, then the speed at which it happened surely should have. Most of the animals in their experiments had become extremely sick by the 8th week of being on a specially designed deficiency diet. By the 8th week, many of the animals were too weak, sick and diseased even to feed themselves. Bizarrely, the researchers resorted to force-feeding the animals for the remaining two weeks of their experiments. The scene in these laboratories must have been something like mini horror torture chambers.
Nonetheless, by the 10th week, nearly all the animals were either dead or very close to dying. That’s correct, in a mere 8 to 10 weeks on the deficiency diet all the animals were very seriously diseased or dead. Needing to force food down a rat’s throat should have been another major clue that there was something drastically wrong with it.
Each animal was fed and watched and after loss of smell occurred, the food was actually placed in its mouth until the ration was consumed. (page 575)
Maybe those lesions on the animal’s tongue (no doubt in the shape of the food pellet too) should have been another clue? Once again, seeing all this disease and destruction in response to a mere deficiency is so completely illogical. What any reasonable, and thinking, person would expect to see in response to a mere deficiency is a slow wasting and general tissue atrophy. After all, this is the response that’s always been witnessed in nature, and witnessed for over thousands of years too, due to prolonged and even complete starvation. Clearly then, there was something else drastically wrong with the artificial deficiency diet used in these lab experiments.
This takes us into the heart of the matter. What in the hell were they feeding these animals? It’s almost always the same diet used in these experiments. Basically, with only some slight variations, here’s the list of ingredients of the de-facto vitamin-A “deficiency” proving diet:
- Casein (“deactivated” milk protein)
- Starch (usually corn starch)
- Salt mixture
- Lard (rendered pig fat)
- Brewer's yeast (or vegemite yeast)
- Distilled water
To understand the rationale behind this diet, the researchers believed that it was deplete only in vitamin-A and that it was complete and sufficient in every other regard. The thinking was that the milk casein would provide adequate protein. The starch provided carbohydrates. The high concentration of salt mixture; well I’m not too sure what the purpose of that was. The lard provided ample fats, and the yeast provided the then known B vitamins. Therefore, even though not ideal, the diet should have been sufficient in sustaining the lab animals in somewhat reasonable health.
Hopefully to you, and any cardiologist you might ask, that’s not exactly a heart healthy diet to be on. Additionally, and as well as being acknowledged by subsequent researchers, this diet is not just deficient in vitamin-A. It is also deficient in vitamins D, B12, C, E, K, other usable fats, important minerals such as zinc, fiber and other essential proteins too. However, for our purposes here, we are not actually too concerned about these other deficiencies either. After all, most of these experiments were conducted on rats, and rats are pretty damn tough animals. Even the small lab ones should have been able to still survive for a quite a while on this diet.
As with regular milk pasteurization, the casein used in these experiments had to be sterilized too. After all, the researchers did not want to expose their animals to harmful bacteria such as salmonella, E. coli, and listeria that could easily be attached to the casein protein.
Somewhat overthinking the process, the researchers had the casein, starch, salt mixture, lard, and yeast combined into portion sized pellets. The pellets were then heat treated in an oven (presumably to further sterilize it). On the one hand, the pelletized food allowed the researchers to more easily monitor and control the amount rationed to each animal. However, on the other hand, it made it impossible for the rats to selectively pick only the ingredients they wanted. Tragically, I think that even the lowly, simple, rat would have soon figured out what not to eat from this meager menu.
Very tragically, essentially this same diet design is used by most follow-on researchers who repeat the experiments and confirm the vitamin-A deficiency results. This is not too surprising though, because this is kind of what you are supposed to do in repeating and confirming experiments. There is a bit of a flurry of others repeating these experiments in the early 1920s, some in the 1930s, ’40s, and even in 1960. They all use the same diet. There are a few tweaks made to it here and there, but it is effectively the same. The same diet yields the same results over and over. Similar experiments are repeated in guinea pigs, rabbits, and even monkeys. Almost all animals fed this diet became seriously diseased, and most died within just ten weeks.
So, there you have it. That’s the artificial diet that proved the vitamin-A deficiency theory. Although not ideal, to the casual observer it looks at least somewhat reasonably conclusive. However, we are not casual observers. We are inquisitive and critical thinkers. Some immediate questions show up here.
Firstly, why use such a complicated diet at all. This artificial diet is such a completely unnatural, and even bizarre, diet to try to feed rats on. When in evolutionary history have rats ever lived on casein, lard, and vegemite? Isn’t it a tad presumptuous to think that this human designed diet is going to be instantaneously adapted to by rats? Additionally, a high consumption of salt and fungus (yeast) is probably just not a great idea for a rat, or anyone else. Therefore, why not just use a simple vitamin-A deplete diet that would be more normal for rats in their natural habitats? What about oh say, nothing except just 100% brown rice, oats and a few peanuts?
But, by far, the most concerning question we need to raise is how could these researchers have been so completely disconnected from the norms in nature? As I was reading the various reports, I was thinking, are you kidding me? All that disease and destruction caused by a mere “deficiency?” I mean, to me at least, that is just so completely ridiculous. Additionally, all this lethal disease occurred in just 10 weeks (2.5 months) because of a “deficiency?” That too is so utterly illogical, because if these animals were so incredibly susceptible to this “deficiency” scenario, then they simply would not be on the planet as a species. It is absolutely impossible for animals to have this vulnerability. One winter would have killed them all off. Therefore, the more obvious questions these researchers should have been asking: when exactly did, these animals become this susceptible to this mystical vitamin-A “deficiency?” Just as importantly, why are these same disease conditions almost never seen in the animals while in nature?
Therefore, it should have been abundantly clear to every single one of the people involved in conducting the experiments that the animals were not responding to a deficiency at all. Nope, no way, not a chance of it. These sick experiments were simply poisoning the animals. The animals were responding to a toxicity and an incredibly powerful toxin at that.
Of course, there were at least a few critical thinkers among the early researchers who suspected something was not quite right. They conducted their own vitamin-A deplete experiments and by using diets of their own design. So, what happened in their experiments? Well, nothing happened.
In these other experiments, their animals did not succumb to the so call deficiency conditions at all. There are reports from Emmett, A. D., and Allen, F. P., in the Journal of Biol. Chem., 1920, and that of Stephenson, M., and Clark, A. B., in Biochem. Journal., 1920 where their animals showed no signs of vitamin-A deficiency.
These reports should have raised a major red flag. But, somehow, they did not. They were simply dismissed as being anomalies and disregarded. Now, if you recall from our golden rules regarding experiments, to any legitimate scientists this should have proven the vitamin-A deficiency theory as very likely being wrong. They now had other diet regiments still 100% completely deplete of vitamin-A, which were not producing the deficiency disease conditions.
the same disease conditions – flashing red lights!
Additionally, there was at least one study conducted using McCollum’s disease inducing “deficiency” diet but with abundant amounts of vitamin-A directly included in it. This study was conducted by S. Mori, of Wisconsin, in 1923.
Mori regards this form of ophthalmia as identical with that produced by deprivation of fat-soluble A.
From Mori, S., Am. J. Hyg., 1923, iii, 99.
In this study, he produced the same disease results. That’s correct, even with vitamin-A included in their diets, the animals still developed xerophthalmia and keratomalacia. This result was not just a red flag; it was full-size flashing red lights with sirens. Clearly, there was something hugely wrong with the “deficiency” theory.
This new information should have been the immediate show stopper. But, not to be dissuaded, the results of this experiment were discarded too, and with a completely unfounded rationalization. This action, of course, is also a clear violation of our golden rules for conducting experiments. You can’t just conveniently disregard results that you don’t like, or have some bias against. Now, once again, to any legitimate scientists, this should have proven the vitamin-A deficiency theory as being completely wrong. It should have made them immediately stop the presses, go back to the drawing board so to speak, and reexamine what was so wrong with McCollum’s disease inducing “deficiency” diet.
Naturally, what S. Mori did in adding vitamin-A back into the baseline diet is a standard practice in conducting experiments, and is more generally termed to be the control experiment. Of course, there are other researchers who do indeed investigate this control scenario of adding back the vitamin-A into McCollum’s disease inducing “deficiency” proving diet. The rational thinking is that if they add back only vitamin-A into the baseline diet, and if the diet then maintains the health of the animals, that would confirm that they’ve isolated it down to just this one “deficiency” factor causing the diseases.
On the surface of it, that sounds perfectly logical. However, it’s not quite that straightforward. This is where we need to remember another golden rule for conducting experiments, and that’s never to change more than one variable at a time. There are several vitamin-A “deficiency” studies from the 1920s that run this parallel control experiment, but they are primarily focused on reproducing the striking disease conditions induced in the eye. Therefore, the one I’d like to reference and discuss in this context is once again is the Wolbach and Howe study of 1925:
TISSUE CHANGES FOLLOWING DEPRIVATION OF FATSOLUBLE A VITAMIN.
From the Department of Pathology, Harvard University Medical School, and the Forsyth Dental Infirmary, Boston.
Received for publication, September 4, 1925
Source: Pharmaceutical Research Department,
F. Hoffmann-La Roche & Co., Limited Company, Basle, Switzerland, 1989 |
What’s so important about Wolbach and Howe’s 1925 study, is that not only is it the premiere study that proved the enormous scope and devastation caused by the so-called deficiency, it is also the study referenced today as being the one to definitively close the case on the vitamin A deficiency theory.
Wolbach and Howe’s 1925 study is probably one of the most comprehensive vitamin-A deficiency studies done in this era. Not only does this study investigate the broader scope and magnitude of the vitamin-A “deficiency” induced disease conditions, it in parallel runs the needed control experiments. My perspective on this study is that it was well designed and well conducted. They conduct rigorous and thorough postmortem investigations of the extent of all the affected organs and tissues. Overall, their report is excellent, and I encourage you to read it in detail. The report completely supports and reconfirms the vitamin-A “deficiency” theory. Additionally, to prevent the complication, or conflation, of follow-on infections, they keep the animal cages meticulously clean and keep only one animal per cage. Actually, ruling out the involvement and contribution infections make in the overall disease picture is one of the key objectives of this particular study.
However, the authors of this study are also very dismissive of the other contemporary vitamin-A-deficient diet experiments that are not producing the disease conditions. From the report’s introduction, they state:
Few pathological studies have been made, and the majority of these have resulted in wholly negative results and, therefore, erroneous conclusions as to the sequence of events and importance of infections.
They then go on to enumerate the other studies that have “resulted in wholly negative results” and attempt to rationalize them away with not much more than a single sentence. Although, this should alert us to the high probability that Wolbach and Howe had some biases. Even still, I don’t really think their apparent biases were a big factor since the results that they were looking at were indeed powerfully compelling. However, they do make a simple, and fundamental, scientific mistake. It’s a deceptively simple mistake. I believe they were led into making this mistake by the accounts of the very earliest researchers using butter and cod liver oil as sources of high concentrations of vitamin-A. As a means of adding vitamin-A back into the baseline diet, they substitute out the lard by replacing it with butter.
Controls.
Control rats on the same diet, but with butter fat (prepared from fresh butter by melting and washing in hot water) in place of lard, grew normally and have been maintained in normal healthy condition for a year.
Not only was their control diet preventing the onset of the disease, but it was also promptly reversing it too.
The control diet was tested for its curative properties, and its administration was always followed by prompt amelioration and disappearance of the signs and symptoms of the deficient state.
Although this sounds like rather fantastically good news because it’s clear evidence that the disease condition was not only caused by diet but that a simple diet change could ameliorate it too. However, and somewhat counterintuitively, we can’t jump to their conclusion that the vitamin-A in the butter was solely responsible either. That’s because the substitution of the butter in place of the lard had not changed just one variable in their control experiment. Not at all. Rather, it had changed at least three variables at the same time. They’ve added vitamin-A, they’ve added vitamin D, and more importantly, they’ve changed the composition of the fat. In 1925, it was more or less assumed that a fat was a fat, and it was thought to just be a source of food energy. The butter fats most certainly could have much better emulsification properties than does lard in regard to the retinoids. Some important differences between butter and lard is that butter has about twice the concentration of cholesterol and saturated fats. Of course, modern medicine and nutritional science claims that higher levels of cholesterol and saturated fats are bad for us. But, please remember that we are now in a negative universe. What we’ve been told is the complete and total opposite of what’s true. In the context of a fat-soluble toxin, such as retinol, the higher density fats are hugely more protective.
But, there’s a hidden fourth variable they’ve changed with this simple butter substitution in place of the lard. It is something they could not have known about. It’s not what they’ve added into the diet; it’s what they’ve taken out of it.
You now have enough information to figure out the mystery here. What was really going on in these experiments? What substance(s) do you know of that can even possibly cause the scope of the disease and catastrophic tissue destruction exhibited in these animals? Additionally, what substance can cause all of that disease to happen so quickly? Of course, it also must be a substance that was inadvertently, and unknowingly, included in the animal’s diets of these experiments. I’ll bet you know its name.
Yes, it’s retinoic acid. The chemotherapy drug. The rats in these experiments were simply chemo’d to death. If true, where was the retinoic acid coming from? Well, there are two sources of it.
What is lard? Basically, it’s pig fat from the adipose tissue of the slaughtered animal (mostly the skin). Lard is produced via a process known as rendering. Rendering is exposing the remnants of the hog’s carcass to high heat or steam and separating off the fat. Although that might not sound too delicious, in the animal processing industry, nothing is wasted.
Here’s where I need to interject with some trivia. Of all the mammals on the planet, there are only about two that are known to collect retinol within the fats of their adipose tissues (the skin). It’s humans and domesticated (farmed) pigs. In most other mammals, there is no detectable retinol in their skin lipids. Of course, pigs are sent to feed lots for “finishing” where they are first deliberately fattened by feeding them heaps of corn. Yes, corn is excellent at fattening the animals, and it is also a very good source of the yellow carotenoid vitamin-A precursor, and it’s a reasonably good source of vitamin-A too. Naturally, us humans (in the domesticated Western world) are continuously at the feed lot eating tons of high vitamin-A content foods too. And, yes, just as with the hogs, we get fat too. With that juicy bit of trivia explained, let’s get back on track here.
Okay, so lard is rendered pig fats, and that fat would normally have significant levels of various forms of vitamin-A contained within it. But, after rendering, lard is reported to have virtually no vitamin-A, or maybe only trace amounts of it. So, what happens to the original quantity of it? Well, it mostly gets separated off into the yellow (yes, retinol is yellow), less market appealing lards. However, the separation process is not 100% perfectly efficient. More importantly, remember, retinol is easily converted into retinoic acid via oxidation. All that’s needed to create the oxidation reaction is heat and oxygen. Ample amounts of both are present in the “rendering” process used to produce lards. Therefore, the lard in these experiments contained retinoic acid. This is not just a theory of mine. We have hard evidence for it. We just need to skip ahead a few decades to another vitamin-A deficiency experiment done in 1953. This study is a fascinating account.
Studies in Vitamin-A
26. THE VITAMIN-A-REPLACING EFFECT OF LARD
In this experiment, the researchers have conclusively determined that there is some mysterious hidden factor in lard that is having the same effects on tissues as does vitamin-A. They conduct a rather extensive investigation trying to isolate this substance. They narrow it down to being in the yellowish constituents of the lard, but are never able to detect vitamin-A.
The lard used yielded 0-23% unsaponiflable material as a very pale yellow, low-melting solid which in concentrated solution fluoresced pale blue under ultraviolet illumination.
A solution of the unsaponifiable material in cyclohexane (8-6%, w/v) was yellow and gave a very pale-green color with the SbCl3 reagent. No absorption band could be detected in this green solution. The absorption curve of lard unsaponiflable material showed inflexions at 225 me. (El% 14-0), 250-300 mμ. (El% 270 mμ. 5-5), 315-365 mμ. (El% 330 mμ. 0-9), 445-460 mμ. (El% 450 mμ. 0-06) and 470-495 mμ. (El% 480 mμ. 0-04).
The unsaponifiable material was chromatographed on watered A1203 (Table 1), but neither preformed vitamin-A nor carotenoid precursors could be found in any fraction. (page 681)
Next, here’s where a bit of chemistry factors into the equation. A standard laboratory technique for detecting certain chemicals is the process of chromatography and fluorescence. When certain molecular structures are exposed to light of very specific wavelengths they will fluoresce (they glow). The color they fluoresce at is also very specific to the molecule. Therefore, the specific combination of the inbound induction wavelengths and the responding emission wavelengths can very reliably isolate specific molecules. Retinol’s absorption wavelength is at about 335 nm, and it’s emission wavelength is at 458 nm.
With this technique and associated equipment, the researchers in this experiment intensely search for retinol in their lard samples. To be clear, this is no trivial effort on their part, because they are almost certain it’s there. After all, they can directly see the influence something like vitamin-A is having on cells. However, the mystery chemical is not to be found. What they were not aware of in 1953 is that retinoic acid is the real heavy hitter in this dynamic duo of retinoids. What they are also not aware of is that retinoic acid does not fluoresce, not at all, not at any wavelength. With the oxidation process of converting retinol to retinoic acid, the molecule’s structure has changed, and that prevents it from fluorescing. Therefore, I believe that the vitamin-A effect they were seeing was that of retinoic acid.
The effects of vitamin-A deficiency on epithelial tissues are so definite that it is reasonable to expect some trace of the vitamin in those tissues which in avitaminosis exhibit the characteristic keratinizing metaplasia. In fact, however, Popper (1941, 1944) and his colleagues failed to discover any evidence for the presence of vitamin-A in the epidermis or epithelium of the mucous membranes, tissues which are considered to be the first sites of vitamin-A deficiency. The fluorescence technique used might well have revealed anything more than minute traces. (page 685)
Other researchers at the same time confirmed that lard does indeed also contain vitamin-A
According to Herb et al. (1953) lard contains 0-5-2 i.u. of vitamin A/g., which is of the same order as that we have found in the beef fat - mutton fat mixture.
By J. GILLMAN, K. BARBARA NORTON, D. E. A. RIVETT AND D. A. SUTTON
Joint Nutrition Unit of the S.A. Council for Scientific and Industrial Research and the University of the Witwatersrand, Johannesburg and
National Chemical Research Laboratory, South African Council for Scientific and Industrial Research, Pretoria (Received 22 August 1955)
Another significant source of vitamin-A in the earlier vitamin-A deficiency experiments would have been the milk protein, casein. Casein acts as a carrier molecule for retinol and highly bonds with it. It normally contains a relatively high concentration of vitamin-A.
See: Binding of vitamin-A by casein micelles in commercial skim milk.
https://www.ncbi.nlm.nih.gov/pubmed/23261375
Of course, the understanding of casein as a substantial source of vitamin-A is not at all a new discovery. McLaren acknowledges this fact in his 1963 textbook. In reference to an early paper by Powers Park in Simmons in 1923, he states:
For example, 1 of the 2 diets containing casein had three times more casein than the other this would be a good source of the vitamin, for special extraction methods were not in use at that time.
Source: MALNUTRITION and THE EYE, forward, page ix
However, if it was just retinol (not converted to retinoic acid) included in the casein, those tough little rats should have been able to tolerate that for a good long while, and much longer than just 8 to 10 weeks. Since retinol is normally found in casein, and these researchers knew that there was none remaining in the “deactivated” casein used in the rat diets, what happened to it? Well, they assumed that the deactivation process had destroyed it. But, no, it was not destroyed. They unknowingly provided the oxidation chemical reaction needed to convert that retinol into retinoic acid. As in the 1950s, back in the 1930s, the standard test for retinol was using fluorescence. At the specific induction wavelengths, retinol fluoresces a nice light blue color. It’s the key indicator that retinol is present. However, after conversion to retinoic acid, the molecule no longer fluoresces, at all. Therefore, they would have been quite certain that there was no retinol remaining in the casein used. But, in 1925, it appears they were not even aware of retinoic acid, nor its properties. Therefore, in their zeal for sterilizing the casein, they converted its included vitamin-A into its most toxic form. From Lowe and Morton’s 1953 report cited above, we have this description of the process they used to “deactivate” the casein used in their experiments.
Light white soluble casein (B.D.H. Ltd.) (400 g.) was boiled under reflux with abs. ethanol (2 1.) for 3 hr. It was then filtered at the pump and twice washed with 200 ml. portions of boiling ethanol. The casein was again refluxed with fresh ethanol (2 1.) for 3 hr., filtered and washed as before. It was then dried overnight at 110 C in an electric oven and on the next day ground to a fine powder and incorporated in the diet mixtures.
Next, we need to consider yet another earlier vitamin-A deficiency experiment done in 1927. They too were conducting control experiments to prove that by adding vitamin-A back into the base line diets it will prevent xerophthalmia and the other anticipated deficiency conditions.
The base diet they use is:
Group/.–(Diet -A-D.) This diet is deficient only in vitamins A and D, and consists of the following:
| Inactivated* technical casein (Merck) Corn-starch Cottonseed oil Salt mixture, McCollum No. 185 (6) Vegex (lVIarmite) (for vitamin B) Decitrated lemon juice (for vitamin C) Distilled water |
20 gm. 50 gm. 15 gm. 5 gm. 5 gm. 5 cc. 50 cc. |
|
|
* By heating and aeration (Goldblatt and Morltz (5)). |
||
From the Department of Pathology, School of Medicine, Western Reserve University, Cleveland. 1927
The key detail here is that they use casein that had been “inactivated” by applying heat and aeration. Of course, using “inactivated casein” is a standard practice in nearly all the vitamin-A deficiency experiments. Here is another example from an even earlier study done in 1923.
The food of the animals on the vitamin-A low diets contained an adequate amount of the various food constituents—protein, carbohydrate, fat, inorganic salts and vitamin B (obtained from yeast). Since the casein which furnished the protein was extracted with hot alcohol for twenty-four hours and ether, U. S. P., for forty-eight hours in a Soxhlet apparatus, and only 10 per cent, of lard was included in the ration, it is obvious that an extremely small amount of the fat-soluble vitamin-A was present in the food.
AMY L. DANIELS, Ph.D. AND MARGARET E. ARMSTRONG, M.D.
WITH THE COOPERATION OF MARY K. HUTTON, B.S.
IOWA CITY 1923
The China Study, or to use the more official name, the "China-Oxford-Cornell Study on Dietary, Lifestyle and Disease Mortality Characteristics in sixty-five Rural Chinese Counties”, was one of the most comprehensive epidemiology studies ever conducted. The study is summarized, and the results analyzed in the book of the same title, by T. Colin Campbell, Ph.D. of Cornell University. I highly recommend this book.9 The takeaway from the study is that much of the blame for the epidemics of our chronic diseases in North America is attributable to our high consumption of animal-based foods; such as meat, dairy, eggs, etc. But, if I could condense Campbell’s great book down to just a couple of sentences, here’s what I think his principal messages are:
- The disease rates in North America is absolutely off the charts in the context of the more normal worldwide rates.
- Our foods are causing our epidemics of chronic disease.
- The worst offenders are the animal sources of protein.
- Either you go vegan, or you are going to die young.
In addition to these messages, Campbell’s other prime conclusion is that the very worst (disease promoting) food from the animal sources is milk, and he pins the blame squarely on the casein protein within it. Naturally, much like in these early experiments, our zeal for sterilizing mass-produced foods, the mandatory pasteurization of the milk permitted in the national milk supply exposes the embedded retinol hidden within its casein protein to high heat. I wonder how much of its retinol gets converted into retinoic acid without us ever knowing it? Very unfortunately, Campbell goes off the rails a bit in his analysis. He mistakenly makes the extrapolation from milk casein being harmful to that of all animal proteins being harmful. That extrapolation is just plain wrong. And it’s quite tragic too because he was so close to getting it correct. Blaming an entire food group was a mistake, and he just needed to dig a little deeper. He would have seen that it’s not an entire food group that’s causing our chronic diseases. Rather, it’s a few select molecules sourced from many different foods (both plant and animal based) that’s causing them.
9 https://www.amazon.com/s?field-keywords=China-Study-Comprehensive-Nutrition-Implications
Like with the work done in the China study, more contemporary research is directly linking the consumption of cow’s milk, and specifically, the casein protein, with the subsequent development of both Multiple Sclerosis and diabetes.
A team of researchers led by Hospital for Sick Children (HSC) senior scientist Michael Dosch has determined that multiple sclerosis and type I (juvenile) diabetes mellitus are far more closely linked than previously thought, including the role cow milk protein plays as a risk factor in the development of both diseases for people who are genetically susceptible.
"Researchers Determine That MS And Diabetes Are Closely Linked Diseases."
ScienceDaily, 22 March 2001.
http://www.sciencedaily.com/releases/2001/03/010322074643.htm
Of course, it’s not just that casein naturally contains vitamin A that makes it a big risk. Rather, it is that the vitamin A is wrapped up in the protein, and that enables it to bypass the body’s normal pathway for storage in the liver. The casein protein wrapper is allowing the retinol molecule to slip undetected beneath the body’s otherwise protective retinol radar, so to speak, and penetrate deeper into these other organ tissues.
The misunderstanding of casein containing vitamin-A back in the early 1920s is reflected in this comment from McLaren.
Elsewhere (McLaren, 1959) reference has been made to the belief, widely held at one time, that it had been demonstrated in the laboratory that diets containing protein of poor quality and deficient in vitamin-A cause xerophthalmia to develop more rapidly than those with good quality protein. Such a statement was made by no less and authority than Parsons (1932), without giving any source, and appears in the fourth edition of “The newer knowledge of nutrition” by McCollum and Simmonds (1929). The original source seems to be a paper by Powers, Park, and Simmons (1923) which describes the feeding of rats on 3 diets, all deficient in vitamin-A and containing protein of different qualities. It is evident that the diets were not equally deficient in vitamin-A. For example, 1 of the 2 diets containing casein had 3 times more casein than the other. This would be a good source of the vitamin for special extraction methods were not in use at that time.
Source: MALNUTRITION and THE EYE, page 110
In the early vitamin-A deficiency experiments, the result was usually the complete transformations of the various epitheliums, and almost always resulted in follow-on opportunistic infections, and following that, death. However, most of these studies from this era were just focused on reporting the striking degenerated epithelial tissues of the eye. The less publicized, yet critically important finding of the experiments was that the so-called deficiency was destroying almost all the epithelial tissues in the body, and almost regardless of what organ or gland it was contained in.
Likewise, and by a wide margin, in Wolbach and Howe’s 1925 study the common theme, and specific tissue most affected by the deficiency was the epithelial tissues. Therefore, this requires us to drill down into, and get a clear understanding of what’s happening with this specific tissue type. Let’s consider some the comments in Wolbach and Howe’s 1925 report regarding what’s happening to the various epithelial tissues.
Mucus is another substance which may be followed microscopically, and inasmuch as the commonest seats of the keratinizing changes are mucus-secreting epitheliums, we have tried to establish some association between the two.
AMY L. DANIELS, Ph.D. AND MARGARET E. ARMSTRONG, M.D.
WITH THE COOPERATION OF MARY K. HUTTON, B.S.
IOWA CITY 1923, page 762
What’s so important to understand here is that not only are the epithelial tissues the primary target of the disease condition, it is the way in which they are affected and respond. What’s observed is the rapid and accelerated mitosis of the basal stem cells.
Mitotic figures are numerous and growth may take the form of a thin layer of cells underlying the original epithelium or of a circumscribed clump.
…
With growth which is rapid, as attested to by the number of mitotic figures, the cells form an orderly stratified layer applied in normal fashion to the tunica propria; the superficial cells exhibit the sequences of normal keratinization as regards presence of keratohyaline globules and staining reactions. Throughout the duration of life, multiplication of the basal layer of cells continues at a rapid rate, and large numbers of keratinized cells are thrown off.
Source: As above, page 764
Seeing rapid and accelerated stem cell division should have been another major clue that they were not looking at a deficiency condition at all. Instinctively, we’d expect the normal response to a severe deficiency condition to be a slowing down, or even stalling, rather than a significant acceleration, in the rate of cellular division. Once again, it should have raised major alarms as to some other hidden force being present in these experiments. Even though it is completely obvious, we can now go through a simple elimination process to pin it down to one root cause. Currently, there are about two known food-based toxins that can provoke stem cells into a rapid replication as seen in these experiments. Additionally, here we have animals in these experiments restricted to an incredibly small number of unique food items. That does not leave us with many possibilities as to who the prime suspects are in causing the rapid stem cell replication. Actually there are only two possible suspects: retinol and / or retinoic acid.
Except, since these scientists had gone to great lengths to eliminate, and ensure, that all retinol was removed from the casein, and lard, that leaves us with one choice. It’s retinoic acid. And, of course, all the disease conditions induced in these animals is a perfect match for the same conditions induced in humans when being treated with retinoic acid. Therefore, I say we go with the highly logical maxim: if it swims like a duck, looks like a duck, waddles like a duck, and quacks like a duck, then it’s probably retinoic acid. Well, you get the point, it is retinoic acid.
Thus, it should be very clear that it was not so much the substitution of butter into the diet that had promptly ameliorated the disease conditions, rather it was the removal of the lard with its hidden retinoic acid. The researchers had simply removed one of the primary sources of the retinoic acid toxin from the diet. Therefore, while being fed lard, the rats were simply being poisoned to death. However, I have no doubt that the higher density fats and cholesterol of the butter helped significantly by emulsifying the retinoic acid hidden within the casein. The beneficial, and protective, aspects of these fats would have far outweighed any additional risk it’s own vitamin-A content may have presented. Regardless, the bottom line here is that these deficiency experiments were utterly botched. Not only did their so-called deficiency diets contain substantial amounts of vitamin-A, it is simply impossible for all of that disease to be the result of a mere deficiency. Seriously, anyone’s grandmother could figure that one out.
Oh; but wait a minute, maybe it was that the animals were deficient in retinoic acid too? Maybe, without retinol, the animal’s cells could not have normally been producing retinoic acid, and therefore they were deprived of its wonders. Well, by about 1959 scientists were getting a better understanding of retinoic acid, and were gleaning some insight into its magic powers to vastly speed up stem cell division. Also, around 1959, it had been determined that vitamin-A would be slowly metabolized to retinoic acid (vitamin-A acid). They also knew that retinoic acid could not convert back into retinal (termed retinene at the time).
In 1960, a research team at Harvard investigated this exact question I’ve just posed. They wanted to know what beneficial effect retinoic acid would have in a vitamin-A deplete diet. Basically, their hypothesis was that maybe animals don’t need vitamin-A so much, rather it is that they needed the downstream metabolite of it. In other words, maybe the animals in the early experiments were shortchanged by not getting enough retinoic acid?
In the Harvard team’s experiments, they still used a very similar (a nearly identical) “sick diet” as the deficiency researchers did 35 years earlier, (things don’t move fast in medical research). They just “supplemented” the diet design with retinoic acid too.
Normally the rat after about eight weeks on a vitamin-A-deficient diet become sick and rapidly dies, at about the same time as the retina is beginning to degenerate. By taking advantage of the fact that vitamin-A asset prevents general tissue degeneration and death, without being reduced in vivo to retinene or the vitamin, which are necessary for vision the Harvard workers (Dowling, 1960) have been able to follow the changes in the retina for as long as 10 months. Figure 14 shows the progressive changes in these animals.
… more
After 2 months on the deficient diet supplemented with vitamin-A acid retina has begun to degenerate.
Source: MALNUTRITION and THE EYE, page 110
Sure enough, the Harvard team got very similar results as before. Although in their experiments some of their animals died less quickly. Nonetheless, their conclusion was, nope, not even retinoic acid could save the animals from the horrors of vitamin-A deficiency. They too were quickly producing xerophthalmia in the animals in just 8 to 10 weeks.
Next, let’s look at the real effects that retinoic acid treatment (when used as an acne drug) has on human vision, and the eye health. Here’s an excerpt from a recent medical textbook documenting the “mild” side-effects of isotretinoin (Accutane et al.). “Isotretinoin” is the more scientific chemical name for retinoic acid.
Mild, transient arthralgias and myalgias may occur with isotretinoin therapy, but these usually do not require discontinuation of therapy. There are also sporadic reports of arthritis responding to dose reduction and Achilles tendinitis.
Effects on vision and central nervous system. In addition to the xerophthalmia commonly experienced, and meibomian gland atrophy and corneal opacities reported with isotretinoin use, photophobia and decreased dark adaptation/night blindness can also occur. The loss of the dark adaptation maybe permanent.
Isotretinoin administration is known, rarely, to precipitate pseudo tumor cerebri, resulting in severe headaches. This side effect is reversible with discontinuation of isotretinoin in conjunction with the administration of a systemic corticosteroid.
Although a causal relationship has not been established, reports links suicidal depression to isotretinoin use even in individuals with no prior history of depression or suicide attempts. In general, nonetheless, that successful treatment of severe acne with systemic isotretinoin can have immensely positive impact on psychological outlook. There is no currently known pharmacological mechanism to account for the psychiatric symptomatology associated with isotretinoin in this issue remains controversial.
Anders Vahlquist, Madeleine Duvic
CRC Press, Jun 20, 2007 – Medical
See page 116
So, wow, would you look at that? Retinoic acid (isotretinoin) is known, and proven to cause xerophthalmia in humans. Also note the exact same condition develops in the meibomian glands in both the vitamin-A deficiency experiments and with isotretinoin usage (the meibomian glands are the sebaceous glands at the rim of the eyelids inside the tarsal plate, responsible for the supply of meibum. The meibum is the oily substance that prevents evaporation of the eye's tear film). So, there you have it, retinoic acid is documented to cause exactly the same conditions in the eye as does so-called vitamin-A deficiency.
Okay, I mean seriously, does anyone think for one second that a mere deficiency is going to have exactly the same catastrophic effects, and have it induced at about the same speed, as being treated with a powerful chemotherapy drug?
All of this should now explain the reason why we have the glaring paradox of vitamin-A deficiency being an exact match for vitamin-A toxicity. It is because they are exactly the same condition. The published symptoms of vitamin-A deficiency are really the symptoms of vitamin-A toxicity and or retinoic acid overdose.
If you want to get a sneak-peek at what really happens to rats after being on a diet completely, 100%, free of vitamin-A for more than ten weeks, here are two friends of mine who can show you.
https://www.youtube.com/watch?v=QjpNIS9g9ZA
Autoimmune disease
In my prior e-book I detailed much of my personal experiences with, and significance of, using fluorescence to gauge the amount of vitamin-A in my skin. It is quite a fantastic tool because you can literally see the vitamin-A glowing in your own skin, and see it with your own eyes. The equipment needed is very low cost and can be used by anyone. The process is not invasive and yields immediate results. Of course, this is not a unique experience to just myself. It is well known about, and has been used as a diagnostic tool in the context of vitiligo. Vitiligo is the “autoimmune” disease that causes the loss of the pigment generating melanocytes from the skin and hair shafts.
An ultraviolet light can be used in the early phase of this disease for identification and to determine the effectiveness of treatment. Skin with vitiligo, when exposed to a blacklight, will glow blue. In contrast, healthy skin will have no reaction.
Source: https://en.wikipedia.org/wiki/Vitiligo
And then this:
Vitiligo is sometimes associated with autoimmune and inflammatory diseases such as Hashimoto's thyroiditis, scleroderma, rheumatoid arthritis, type 1 diabetes mellitus, psoriasis, Addison's disease, pernicious anemia, alopecia areata, systemic lupus erythematosus, and celiac disease.
Source: Same as above
That’s correct, they can literally test for and see the elevated levels of vitamin-A in the skin, and it correlates with all the above so-called autoimmune diseases. Obviously, it is not just the diseased skin that’s “reacting” with blue florescence, rather it is a molecule within the diseased skin that’s fluorescing. But, here’s the clincher detail. Many young people in Africa are now directly inducing the vitiligo condition in themselves to whiten their skin. They are doing this by taking isotretinoin (the same drug as Accutane and otherwise known as retinoic acid), or applying it topically. That’s correct, these people are directly inducing the vitiligo “autoimmune” disease in themselves using retinoic acid. It’s the result they very misguidedly think they want to achieve. Of course, what the toxic drug is really doing is killing off stem cells all over the body too, and not just the pigment producing melanocyte stem cells of the skin. The long-term result will be devastating for many of these people, and many undoubtedly will die early and painful deaths because of it too.
high dose retinoic acid
It is tremendously, and critically important to understand that these early experiments (1913-1927) are the same ones that definitively proved the existence of vitamin-A “deficiency.” That’s right, based upon these official experiments, the theory of vitamin-A “deficiency” was thought to be proven, reconfirmed and solidified. Vitamin-A was then crowned and given the center podium in the prestigious vitamin club. But, we now know better. The irony of the situation could not be greater. That’s because the so-called vitamin-A “deficiency” theory was proven by poisoning animals with the most toxic form of it. Therefore, retinol has never been proven to be a vitamin. Therefore, vitamin-A is not a vitamin at all. It has been an imposter foisted on us by bad science for over 100 years.
However, it is crucially important to understand that the disease conditions expressed in these early animal experiments formed the basis of how modern medicine now recognizes thought to be vitamin-A “deficiency.” When these same conditions now exhibit in people, it is often quickly diagnosed as vitamin-A deficiency. And, of course, why wouldn’t it be? Xerophthalmia is the primary example of this.
However, it goes way beyond that. For example, let’s consider Alzheimer’s disease. What’s now being reported,10 is that many patients with Alzheimer’s are also presenting the co-morbidity symptoms of so-called vitamin-A “deficiency” too. But, it’s not that the Alzheimer’s researchers are making the wrong determination. They are simply making the correct determination, but it’s based on the wrongly defined vitamin-A “deficiency” symptoms. It’s the very foundation of the definition of the vitamin A “deficiency” symptoms that’s wrong. Naturally, as I’ve claimed in my prior e-book, Alzheimer’s disease (the brain symptoms) and its presentation with all the co-morbidity symptoms of the thought to be vitamin-A “deficiency” are really the end result of long term vitamin-A poisoning.
10 http://www.nhs.uk/news/2017/01January/Pages/Vitamin-A-deficiency-linked-to-Alzheimers-disease.aspx
You really need to appreciate the significance of what’s been presented in this chapter. These botched experiments no more proved that retinol was a vitamin than did they proved cyanide to be a vitamin. I believe that I’ve presented sufficient information to at least suspend retinol’s membership from the prestigious vitamin club. I have zero doubt that with time, it will not only be permanently kicked out of the club, but it will also be exposed for what it truly is. It’s a cytotoxin that has killed and diseased untold millions of people.
In the next chapter, we are going to step out of the artificial world of the laboratory and take the vitamin-A deficiency theory out into the light of day. We are going to test it in the real world. We’ll find out what really happens when people, and animals, are exposed to chronic and long-term vitamin-A deficiency.
In this chapter, we are going to conduct an in-depth and logical and physical examination for evidence of vitamin-A deficiency in the real world. Of course, it is going to be a bit problematic because we now have no proven or known symptoms of true vitamin-A deficiency to measure or identify it by. Nonetheless, we’ll do our best to make sense of what evidence there is.
Surely, if there is truly such a thing as a vitamin-A deficiency, and we are all so easily vulnerable to it, then we should be able to find numerous examples of it happening in people around the world. Of course, we are told this is hugely the case in South East Asia and Latin America where vitamin-A deficiency is reported to be endemic. However, once again, these reports are based on the field workers in these regions seeing the same documented symptoms induced with the botched science of the earlier animal experiments now showing up in people. Of course, when Western doctors working in Southeast Asia see kids with xerophthalmia, and / or night blindness they immediately attribute it to, and conclude, it’s vitamin-A deficiency. For most of these doctors, there are absolutely no doubts about it. And why would there be, since it’s literally the textbook defined definition of it? Sadly, for the diseased kids, it is exactly the opposite. Xerophthalmia and lesions on the eye are the symptoms of vitamin-A poisoning, and even that of retinoic acid poisoning (with sunlight and infections being significant contributing factors). So, is this truly vitamin-A deficiency they are seeing in these regions? The shockingly simple answer is, no, it is not. This is not my opinion; it is a fact.
The evidence for this is that the widespread so-called vitamin-A deficiency conditions in these regions are not reported in their long histories. If vitamin-A deficiency really existed on a wide scale in these countries, it would have been well documented and written about. Yet, there is no record of that that I could find. There are only a scant few references to blindness. Do you think people say 1,000, 500, 200, and 100 years ago would not have noticed great swaths of their populations going blind, and dying from all their skin mysteriously burning off? I’ve found no record of this at all. There are records of great plagues (infections), starvations, floods, and wars. But no records of widespread disease that sounds even remotely close to being attributable to vitamin-A deficiency. Can you imagine in the thousands of years of their documented histories, that there is no mention of the worst disease condition in their countries, one that burns the eyeballs out of children, being not written about?
Moreover, with the devastating effects that so-called vitamin-A deficiency has on both the male and female reproductive organs, how is it that India and China have built up to their billion person populations? How is it that these populations were doing just fine, and doing quite fine for the last 5,000 years too without vitamin-A supplementation? How is that the “endemic” regional vitamin-A deficiency has only shown up in the 20th century after we discovered the existence of vitamin-A, and had a product to sell them? However, this is just the starting point in revealing just how ridiculous the so-called vitamin-A deficiency theory is.
Now, here’s the kicker. We are told that vitamin-A deficiency is endemic to SouthEast Asia and that hundreds of thousands, if not millions, die every year from it. The key symptoms used to diagnose vitamin-A deficiency in SouthEast Asia are night blindness, and xerophthalmia (chronic dry eyes). In a later chapter, we’ll dig a whole lot deeper into the vitamin-A supplementation programs going on in SouthEast Asia, and South America. For now, let’s just consider the extremely conflicting large scale evidence being presented in North America using these same symptoms of night blindness and xerophthalmia as our measure.
Xerophthalmia: Dry eyes. Xerophthalmia can be associated with systemic diseases, such as Sjogren's syndrome, systemic lupus erythematosus, and rheumatoid arthritis; deficiency of vitamin-A; and use of some medications. It results from inadequate function of the lacrimal glands, which produce tears. When xerophthalmia is due to vitamin-A deficiency, the condition begins with night blindness and conjunctival xerosis (dryness of the eye membranes), progresses to corneal xerosis (dryness of the cornea), and in its late stages develops into keratomalacia (softening of the cornea). Treatment depends on the severity of the condition and ranges from artificial tears and ointments to plugging of the tear ducts. Also known as conjunctivitis arida.
So now, with xerophthalmia, and night-blindness being the de-facto disease conditions attributable almost uniquely to vitamin-A deficiency, and with North Americans being hugely dosed up on vitamin-A since at least the late 1970s, we should expect there to be incredibly few incidences of the diseases here. Not only is vitamin-A supplementation legislated into our staple food products such as dairy and margarine, but it is also commonly added to the flour, and breakfast cereals in the USA. We now eat huge amounts of high source fruits and vegetables year-round too. Even more importantly, on a per capita basis, we are one of the world's highest consumers of pre-formed vitamin-A from animal sources, such as meat, dairy, eggs, fish oils, and liver. Therefore, it is simply impossible for the average person in North America to be even remotely close to being vitamin-A deficient. Seriously, just based upon the historical diet of humans on the planet, the North American diet probably now has at least 100 to 1,000 times higher levels of vitamin-A consumption compared to that of just a few hundred years ago.
With that knowledge, we should expect the rates of xerophthalmia, and night-blindness in North America to be somewhere between micro-minuscule and completely non-existent. But, remember, we are in a negative universe here when dealing with vitamin-A science, and the funny thing is; it’s completely the opposite. It’s just a wee bit tricky. Because here in North America, the same condition is not generally called Xerophthalmia, rather it’s called “Dry Eye Disease.” You see, our doctors here can’t call it xerophthalmia because it does not fit with the narrative of vitamin-A deficiency. Xerophthalmia is just far too closely associated with vitamin-A deficiency, so much so that the incidence rates of xerophthalmia and Night-Blindness are used as a gauge of vitamin-A deficiency in populations. Therefore, physicians here need to call the conditions “Dry Eye Disease” or “Dry Eye Syndrome.” What’s the real difference between the medically defined disease of xerophthalmia and “Dry Eye Disease” or “Dry Eye Syndrome?” Not much at all, they are on the same spectrum, so it just comes down to someone’s opinion. Not surprisingly, even though there is “only” about 200,000 people officially diagnosed with full-blown xerophthalmia each year in North America, the other (but the same) conditions of “Dry Eye Disease” or “Dry Eye Syndrome” are incredibly common here.
Dry eyes are very common, and dry eye syndrome is a major reason for visits to the eye doctor. A recent online poll revealed that nearly half (48 percent) of Americans age 18 and older regularly experience dry eye symptoms.
Source: http://www.allaboutvision.com/conditions/dryeye-syndrome.htm
Also see: Prevalence of Dry Eye Disease among US Men: Estimates from the Physicians’ Health Studies
Of course, there’s a huge disconnect and problem revealed with this information. That’s because it is simply impossible for almost anyone living in North America to be suffering from vitamin-A deficiency, let alone for 50% of the entire population being vitamin-A deficient. When compared to the rest of the world, we have huge amounts of vitamin-A in our diets, yet we have at least 4 million people with serious xerophthalmia, umm, oh, I mean “Dry Eye Disease,” and about 150 million people with intermittent “Dry Eye Disease.” How can that be possible?
Not surprisingly, the same sleight of hand shell game is applied to the terminology used to report the conditions of blocked meibomian glands. Remember, the blocked meibomian glands is one of the premiere and earliest conditions used in the determination of vitamin-A deficiency. However, since almost no one in North America can be vitamin-A-deficient, it can’t be associated with that, so here the condition is called Meibomian Gland Dysfunction11 and given the nice official-sounding acronym “MGD.”
But, if someone in North America is diagnosed with xerophthalmia, then the blame is often put on the person’s accompanying autoimmune disease. That’s right; we are told their mysterious autoimmune disease is magically causing their xerophthalmia syndrome too. There is this almost ridiculous circular blame game going on in an attempt to rationalize away the obvious. In no way is xerophthalmia a complication of these suggested other systemic diseases, such as Sjogren's, lupus, and arthritis. Obviously, the root cause of Sjogren's syndrome, lupus, and arthritis is the same of that of xerophthalmia. Rather, they are all the complications of vitamin-A poisoning! And, of course, xerophthalmia is xerophthalmia, regardless of what continent you happen to live on. Therefore, it is mathematically impossible for xerophthalmia to be caused by vitamin-A deficiency. The emperor wears no clothes.
Sadly, what we now know is that the same thing is causing both xerophthalmia and their comorbidity autoimmune diseases; it’s vitamin-A toxicity. Therefore, the xerophthalmia diagnosis by North American physicians is the perfect example of not seeing what should be blindingly obvious.
11 http://www.allaboutvision.com/conditions/meibomian-gland.htm
Now, if you happen to be still clinging to the notion that xerophthalmia in the developing countries has some connections with vitamin-A deficiency, then here’s a tidbit of information that should clear up any misunderstandings. Xerophthalmia is seasonal. That’s right; it is much more prevalent in the summer months. If xerophthalmia were a deficiency disease, then we’d expect the complete opposite. The summer months provide more fruits and vegetables and therefore provide more vitamin-A in the mostly plant based diets of the “endemic” regions. The summer also provides more green grass for grazing cows and goats, leading to more vitamin-A in their milk. So, why is there this very distinct increase in xerophthalmia during the summer months? The answer is hinted at by what M. Mori of Japan reported in 1904, and what Bloch reported in 1909. Both these physicians reported xerophthalmia showing up in the children in the months of more sunshine. They also both reported that the kids in their care were photophobic (avoided the sun). Vitamin-A is an incredibly efficient light-absorbing molecule. When a kid with elevated retinoid levels in the skin, and /or in the outer tissues of the eyes, gets a bit too much sun, boom, they very quickly pull a great deal of light energy into the tissue, causing it to heat up differentially, and that kick starts the destructive chain reactions. If a very young child in this condition of elevated retinoids makes the mistake of looking directly into the sun for more than just a few seconds, they are in even bigger trouble.
Next, we are going to consider what really happens when people are forced to endure long periods of chronic starvation, and diets completely void of vitamin-A. The prisoner of war camps during the second World War provides us with ample examples. Both the German and Japanese camps maintained hundreds of thousands of people under conditions of extreme starvation. For now, we are going to particularly focus on the Japanese run camps, because it is well documented that the only rations allotted to the men captive in these camps was one cup of rice per day. Additionally, with the fall of Singapore and Hong Kong at the very start of the Pacific war the Japanese had captured about 190,000 British and allied troops. These men (the ones that survived) were captive for the entire duration of the Pacific war, so that’s for about 3½ years. For the most part, they lived on nothing more than one cup of rice per day, and that’s if they were lucky. That’s it. Almost no protein, no fruits and vegetables, nothing else. In addition to the meager single rice ration, the men were forced into hard labor for twelve hours per day. That’s just the beginning of the gruesome conditions and horrors these men were subjected to. Many were brutally tortured, beaten, and exposed to all kinds of infections, had no medical care, were broiled in the sun, and lived in atrocious sanitation conditions. Not only were they exposed to extreme physical and nutritional stress, but they also had to endure extreme mental stress too. It was not just being captive, there was the constant threat of executions, sometimes by being beheaded.
Clearly, for most the men held in these camps they were not only extremely malnourished in all manner of essential proteins, fats, vitamins, and minerals, they had no vitamin-A whatsoever. This was undoubtedly the perfect conditions to induce widespread diseases and infections. Therefore, under these conditions and according to the VAD theory, every one of these men should have quickly gone blind and had all of their epithelial tissues, and therefore all of their internal organs and glands, completely and quickly destroyed. There should have been massive and widespread cases of xerophthalmia, and blindness reported. It should have been almost ubiquitous within the prisoner populations. Obviously, that was clearly not the case. Not only did that not happen, but it was also nearly the complete opposite. Upon liberation, many of these prisoners were examined by Western medical teams. What’s reported should have been, and to a certain extent was, downright astonishing. The eyes and vision in the men remained in exceptional health. The doctors made special notes of how perfect the eyes appeared in most of these men. The sclera was remarkably void of any vascularization (a condition that normally occurs with xerophthalmia), and was perfectly white. American doctors reported the same (very noticeable and surprising) findings in the men liberated from the German P.O.W. camps.
How can that be? These men were chronically starved for years, and many starved to the brink of death (and of course many did die). They probably did not consume even mere specks of vitamin-A for more than three years, and there were almost no signs of vitamin-A deficiency reported. These camps were huge, the Japanese camps each had something like 3,000 to 5,000 surviving men. The German-run camps had 10,000 to 30,000 prisoners each.
|
||||
|



Seriously, you can (and must) see this for yourself. Just get online and look at the pictures of survivors from WWII P.O.W. camps, and even from the German death camps. You’ll see men starved down to being nothing more than mere skeletons. But, please look very carefully at the eyes, and look very carefully at the skin. There are no lesions in the eyes. There are no lesions on the skin even after living in conditions of horrid sanitation. In many pictures, the men are looking directly into the camera too. Figure 8a is just one example.
Do you see any lesions on their skin? Likewise, Figure 8b is another photo where the man is clearly looking directly at the camera.
Shown in Figure 8c is a photo of men, with Private Leo Ayres in the foreground, newly liberated from the Japanese camps who were reading the newspapers about the war having just ended. The point is that you need relatively good vision to read a newspaper.
Shown in Figure 9 is a bit of a zoomed-in view of the faces of men from a German concentration camp. You can clearly see the whites of their eyes (please see the original photo for a better view).
Figure 10 is a close-up photo of survivors from Dachau. Once again, please see the original photo for a better view of their eyes.
These young men are looking at the camera, and you can see the white sclera of the eyes. Even though their bodies have been horribly emaciated down to just living skeletons, remarkably they too have no lesions on their eyes and upper bodies. How can that be possible? According to the vitamin-A deficiency theory, they should be completely blind, and have all of their skin burning off from head to toe with bleeding and infected lesions. As should be all of their internal organs too. Once again, do you see any evidence of that here?
Additionally, this complete lack of vitamin-A deficiency symptoms is not just observable in the men that survived these horrors, its observable in the corpses of those who did not. You can find pictures from the Nazi death camps showing piles of corpses stacked up like cord wood. Clearly, almost all of these victims were horribly starved, and presumably many did die of starvation too. Look very closely; what is it that you don’t see in those photos? For most of them, there are no lesions on the skin.
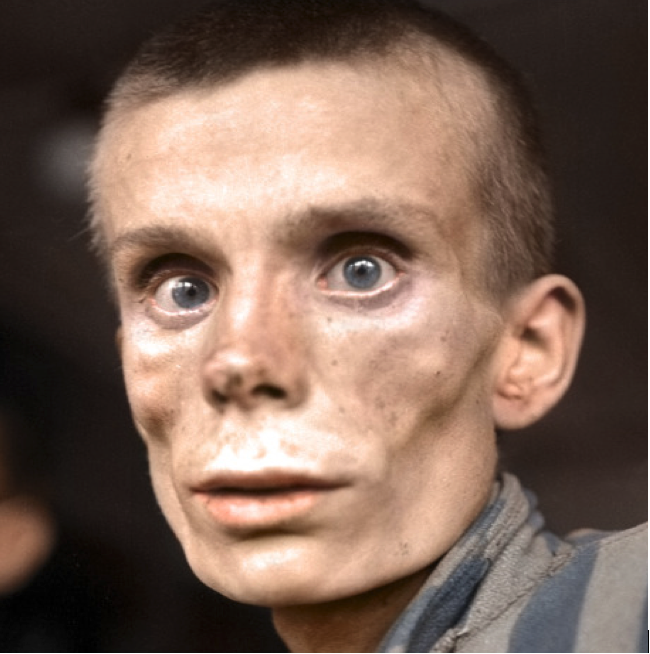
Figure 11 The eyes of a starved Russian man from
the Dachau Camp |
Now, of all the pictures that I looked at, one really stood out for me. Figure 11 is a picture of a young Russian man who’s been in the German Dachau camp for an extended period.
Although the caption on this photo states the person is a Russian woman, I believe it’s a young man’s face. Clearly, he’s been starved for a long while. His eyes are sunken back into the skull. But since this picture has been taken so close up to the man’s face we have a good view of the health of his eyes. Don’t those eyes look remarkably healthy to you? You can see that they’re moist and have no lesions. There’s no vascularization of the sclera. Just as importantly, his glistening eyes are mirroring the image from behind the photographer. You can see in his eyes the reflection of a structure in the background. The light is being reflected off the eyes because they are moist and protected with the tear film. Clearly, this young man’s meibomian glands are functioning just fine. Once again, please remember that the meibomian glands are one of the first to become blocked, and the most commonly affected glands, and as documented on the xerophthalmia spectrum to fail early due to vitamin-A deficiency. Likewise, there are no lesions on this young man’s face. On the contrary, his skin looks to be in remarkably good health too. How can that be?
McLaren summarizes some of these observations in his 1963 text.
During and immediately after the second world war, much greater attention was paid to the medical aspects of starvation and recovery therefrom. Generally speaking, disorders of the eye did not find a prominent place in these accounts.
When the resistance shown by the eyes of experimental animals to total inanition is recalled, this is what might be expected. In their monumental work on experimental human starvation, Keys and his colleagues noted no important deterioration in any sensory function after six months of semi-starvation. They do however state that the sclera and conjunctiva were unusually devoid of blood vessels, the whites of the eyes resembling unglazed porcelain and failing to redden even when soap solution was applied.
Source: MALNUTRITION and THE EYE, page 158
The makeup and structure of the eye is very similar across most species of mammals. The proteins of the eye are also not species specific. The primary nutrients found in, and making up the eye, are proteins, and the B and C vitamins. Of course, we’ve been bamboozled into thinking that only the human eye needs massive amounts of vitamin-A. That’s right, we are supposed to believe that after more than 100 million years of evolution on the planet we humans are the only species that need to supplement with vitamin A to prevent our eyes from self-disintegrating. That, in itself is just so absurd, that it’s almost laughable. Sadly, it’s not laughable because it is a big fat lie that’s at the root cause of our chronic diseases.
Of course, this big fat lie needs to be kept secret. If we were to learn that the human eye has the same structure, protein composition, and therefore the same nutrient needs as in most other mammals, we might question why it is that only humans need to supplement with vitamin-A. How is it that all animal species on the planet can endure prolonged periods of starvation and yet retain perfect eye health and humans don’t? According to the vitamin-A deficiency theory, we should see entire herds of animals on the great plains of Africa and in the Canadian Artic all dropping dead at about the eight-week mark into the dry seasons. All of them should have their eyes disintegrating, and their skin burning off, infected, and all their internal organs failing at about the same time too. Hopefully, you see just how ridiculously absurd that whole notion is. However, I needed to find a well-documented account of an animal kept in starvation conditions for a long period. This brings us to the wonderful and heart touching story of Judy the English pointer that loyally went to war with her owner. Judy was taken into captivity along with her owner, named Frank Williams, a young British navy man at the fall of Singapore in the spring of 1942. This account is documented in the book titled: Judy: The Unforgettable Story of the Dog Who Went to War and Became a True Hero, by author: Damien Lewis, published in 2014.12
Along with Frank, Judy spends the next 3½ years in a Japanese prisoner of war camp. She was even designated an official P.O.W. and given an identification number by the Japanese. Of course, being a dog, Judy was allotted no food and was only able to survive by men donating small portions of their own meager rice rations per day, the occasional piece of boot leather, and whatever she could scavenge. Therefore, Judy survived on not much more than one-third cup of rice per day. Much like the British POWs trapped in these Japanese camps the dog starved down to nothing more than mere skin and bones by the end of the war. So, that’s about 3½ years of chronic starvation. To appreciate just how horrid, and desperate the conditions in these camps became near the end of the war here are some highlights of the story. When the men became too sick and feeble even to walk they were left in their bunks to die. They were not allotted any rations, not even two grains of rice per day could be spared on them. For these men, their only potential source of food was just the flies that they might catch. For the other men in the camp who were still able to walk, they resorted to picking and eating maggots from the latrine as their source of food. The thing is, to catch flies and pick maggots you still need to have good vision.
At this late stage of the war, of course, Judy the dog was allotted absolutely nothing and was viewed as a potential meal to the then also starving Japanese soldiers. Therefore, this dog was not only chronically starved for a very long time; she starved to the near brink of death. Nonetheless, Judy had survived at least 180 weeks being almost completely void of any vitamin-A in her diet. That’s at least 20 times longer than what we should expect based on the vitamin-A deficiency theory and supporting experiments.
Yet, when reading about the very final days in this camp, there is no mention of xerophthalmia or eye disease developing in this dog, or the men. There is a passage in the book, as the men are digging what is presumably their own designated mass graves, they look up at the sky and identify high-flying American bombers on route to Japan. Once again, a person needs rather good vision to identify high flying planes. For Judy to make her final escape from the camp, she needed to perform a feat of remarkable mental and physical dexterity. She remained hidden back in the barracks as all the men lined up to be put on trucks. Frank had quickly trained her with a special hand signal just for this purpose. When signaled, she needed to come running and jump into a sack at the very last moment as the men boarded the trucks. You know what? She needed good vision to accomplish that little feat.
The lifelong bond formed between Frank and his dog is a rather incredible story. Damian Lewis has documented much of Judy and Frank’s experiences during their captivity, and some of it in the post-war period. There’s not one word of mention of Judy having developed any disease of the eye, skin lesions, or of any internal organs that had failed. How is that possible for this dog to have not developed xerophthalmia or any other symptom of vitamin-A deficiency? Of course, there’s only one explanation. Vitamin-A deficiency is a giant myth, if not a big fat steaming pile of lies with maggots crawling through it!
12 https://www.amazon.ca/Judy-Unforgettable-Story-Went-Became/dp/1623656672
There have been several studies attempting to induce vitamin-A deficiency in humans (using volunteers), and it has never really been successful. Meaning, the volunteers just lost weight, and remained healthy, even after more than three years of being on near zero vitamin-A diets there were no signs of vitamin-A deficiency. Various strategies and menus were used in these experiments but for the most part what the researchers found out is that it is rather difficult to induce vitamin-A deficiency in humans. These studies were quietly ended. Nothing to see here, move along.
Probably the most famous of these experiments is the Sheffield experiment. Here’s McLaren’s summarization of it:
None of the 23 volunteers in the experiment carried out by the medical research Council and Sheffield, England who received a diet deficient in vitamin-A for periods ranging from 6½ to 25 months developed any change in the conjunctiva. In adults and older children, therefore in whom the deficiency progresses slowly conjunctival xerosis is not an early sign and for this reason plasma levels and the dark adaptation test, which may be readily carried out in these subjects, are of more value but have their own distinct limitations.
Source: MALNUTRITION and THE EYE, page 171
And then a bit later:
The results of the Sheffield experiment show that very exceptional circumstances are necessary before really marked evidence of vitamin-A deficiency occurs. Even in far Eastern prisoner of war camps where malnutrition deficiencies were rife, xerophthalmia was not usually encountered.
Source: MALNUTRITION and THE EYE, page 208
This brings us to another fascinating account from 1969 of thought-to-be vitamin-A deficiency deliberately self-induced in a person.
Proc Nutr Soc. 1973 Dec;32(3):105A-106A.
Vitamin-A and epilepsy: a dietary contretemps.
Sharman IM, Stern G.
This is an account of a young man who has had epilepsy from the age of twelve, and routinely (about once a month) experienced epileptic seizures. At age twenty, doing his own research on the destructive action vitamin-A has on cell membranes, he’s concluded that his epilepsy was likely caused by some form of subclinical vitamin-A poisoning damaging his nervous system. Based on this determination he goes on an extreme diet of zero vitamin-A and zero carotenoids too. He maintains this diet for more than five years. Remarkably, this strange diet does indeed cure his epilepsy. In this five-year period on his vitamin-A deplete diet he has had only one epileptic seizure, and that’s at the very start of it. But, after five years he is reported to have developed xerophthalmia and a strange gray skin condition. Although he’s been on his strange diet for five years and he’s reported to have the lowest serum levels of vitamin-A ever recorded in Great Britain, it’s between 4.1 µg/100ml and 7.8 µg/100ml. Therefore, somewhat amazingly, even after 5½ years of having no vitamin-A in his diet, some small amounts of it remains in his serum.
Also, remember that we now know that the documented symptoms of vitamin-A deficiency are really those a vitamin-A toxicity. Therefore, his eye and skin conditions could’ve been the result of a lack of fats in his diet. Also, he may have been missing out on other essential nutrients such as proteins, and the B and C vitamins, and zinc.
His doctors spend an extensive amount of effort trying to convince the young man to take vitamin-A supplements to treat his condition. They warn him that if he continues his foolish diet, he will eventually go blind. Even in the face of that threat, he decides to continue his diet. It’s not until his condition significantly worsens that he, very reluctantly, finally agrees to the treatment. He is treated with cod liver oil and his strange skin conditions, and his eyes quickly recover. His physicians, of course, attribute this quick recovery to the vitamin-A in the cod liver oil, and not the oil itself. After the young man has recovered, he immediately goes back to his strange diet of consuming no vitamin-A. I’ve not been able to find a long-term follow-up report of what happens to him after that.
Nonetheless, the material fact here is that he cured his epilepsy with a vitamin-A deplete diet. This fact did indeed spark at least some interest from a few folks in the medical community. After all, curing one’s epilepsy is no minor accomplishment. There is a small follow-up study conducted with eight other people with epilepsy, and they are all placed on vitamin-A deplete diets. There are two remarkable findings from this follow-up study. Firstly, all eight people recover from their epilepsy. That’s an astonishing 100% success rate. Is there any medical drug that has anywhere near a 100% success rate in treating a disease such as epilepsy? The second very noticeable observation made in this experiment is that all eight of these people quickly lose significant amounts of body fat. Therefore, I believe this is pretty clear evidence that vitamin-A consumption is causing the body to retain fat.
I’m not sure why, but the second study is quietly ended and scoffed off as being a case of dietary contretemps. Maybe, it’s because the medical professionals viewed the rapid drop in body fat is a negative response. Or maybe it was because Sharman was one of the most preeminent authorities on vitamin-A, and a big proponent of the grand vitamin-A deficiency theory that he just could not deal with the conflicting real-world evidence, and decided to sweep it under the rug so-to-speak. Moreover, of course, there’s no money to be made in curing people of epilepsy if they only need to make a simple diet change. One other noteworthy comment here is that in the original study it is clearly stated that this young man was on his vitamin-A deplete diet for 5½ years. However, when Wolf13 recounts this case in a follow-up summary report, he states that it’s only four years. I have no idea why Wolf dials back this timeframe number either. Maybe he too just couldn’t deal with the fact that a human can go for 5½ years with no vitamin-A? Yes, that 5½ year number certainly places a lot of doubt on the vitamin-A deficiency theory. The other highly suspicious thing about Wolf’s report is that he claims the vitamin A deficiency experiments can’t be repeated on humans because it would be “unethical”.
Next, we need to ask how vitamin-A toxicity can cause epilepsy? Well, we sure don’t have to look very far and long for evidence. From the so-called vitamin-A deficiency (really vitamin-A toxicity) studies we know that one of the observations was the peeling and disintegration of the myelin sheaths surrounding the nerves. Having this protective epithelial structure peeling off your nerves could definitely cause the epilepsy condition. Moreover, having nerves directly exposed to a molecule that can surprisingly produce an electric voltage could most definitely cause a weird nerve stimulus.
Naturally, this “dietary contretemps” story very much resonated with me. Because I too quickly concluded that my eczema was none other than vitamin-A poisoning. Secondarily, when I first went on my vitamin-A elimination diet, even though I was consuming at least 3,000 calories per day, and with lots of fat, I was dropping weight like crazy. Within about six months I went from being a pretty pudgy guy down to having a completely normal BMI. This ranking is also on the old normal BMI scale, and not the updated version of the scale that is currently being adjusted for the new normal of chunky people.
Not only was I dropping body fat, but somewhat remarkably my muscle strength was also strangely getting better at the same time. Now, after over three years of being on a vitamin-A deplete diet my BMI is still normal, but my muscle mass has gotten greater. I now have a body that looks like what a normal human male is supposed to look like. I most certainly did not drop this body fat because of some malnutrition. No, it was clearly that my body simply no longer had a need for it.
Okay, with all the above evidence, I think we can now see what really happens when people, and animals, are exposed to chronic and long-term vitamin-A deficiency. That’s right, nothing adverse happens. Ironically, they can even get healthier.
13 The Experimental Induction of Vitamin A Deficiency in Humans
George Wolf Department of Nutritional Sciences and Toxicology,
University of California, Berkeley, CA 94720-3104
In this chapter, we are going to analyze the on-going supplementation programs being undertaken in Southeast Asia and South America.
We are told that these large-scale programs are necessary to save the hundreds of thousands, if not millions, of kids who would otherwise surely go blind or die. However, once again, please remember that the vitamin-A world is in a negative universe. What you are about to learn, is that no, the supplementation programs are not saving kids. Rather, it’s the complete opposite. The supplementation programs are causing them to become diseased, go blind and even killing many of them. I believe it’s sterilizing their parents too.
Although we now know that the thought to be a vitamin-A deficiency (VAD) is, in reality, vitamin-A toxicity, we’ll gloss over that little fact here in our analysis of the supplementation programs. Since that’s a new bit of information, we’ll just go with the established VAD theory for much of this chapter.
Of course, in Western medicine, the concept of VAD has been so completely accepted, and so deeply entrenched in the medical thinking that no one even dares to question it. VAD and xerophthalmia are nearly synonymous in medical science. If a doctor now sees a person with a lesion on the eye or other related symptom, they’ll probably immediately suspect VAD. But, as I’ve stated before, the funny thing is; it depends on what continent the person lives on. If they live in Southeast Asia or in South America, then it is surely VAD. And who’s to blame these Western medical doctors for making this diagnosis. After all, it is based on the official science and definition of vitamin-A deficiency. That official definition has been parroted and documented in many medical textbooks by eminent Ph.D.’s on the topic.
However, if any proponent of these programs bothered to do even a few hours of research on the topic, they would quickly discover that it is nearly impossible for the people of these regions to be VAD. The thing is, nearly every food on the planet has some content of vitamin-A or vitamin-A precursor. Many of the green leafy vegetables have very high concentrations. Moreover, many spices are incredibly high in vitamin-A too. A mere pinch of parsley, chives, mint, paprika, oregano, thyme, and red pepper flakes, even once every other month would provide people with ample amounts of it. In many regions of South America sweet potatoes are popular, if not a staple food, and they have very high concentrations of vitamin-A too. The same goes for tomatoes, and bell peppers. Nearly all fruits and vegetables have at least some vitamin-A. As of course do eggs and most meats. Therefore, for the clear majority of the people in these regions, they can easily be getting ample amounts of vitamin-A in their regular diets. Of course, I am not the only person of this view:
A large number foods contain substantial amounts of either vitamin-A or carotenoids, and many these foods are widespread and inexpensive even for the very poor. Thus, in the logical sense, no reason exists for a vitamin-A deficiency to be a worldwide problem. But it is a worldwide problem.
James Allen Olson 1994
Of course, James Olson (a contributor to Sommer’s book) is absolutely correct. With vitamin A (or one or more of its precursors) being nearly ubiquitous, and found in almost every food on the planet, how could anyone be deficient in it. The only way for anyone to not get enough vitamin-A (assuming they need any of it at all) is for them to be eating nothing but rice or beans, three meals a day, seven days a week, and 365 days of the year. Oh, and they have been doing so for five or more years too. How many people do you know that fit into that dietary category? Of course, there’s another dietary scenario that would do it, and that’s one of complete starvation. But, obviously, to a kid facing complete starvation a shot of vitamin-A is not going to do very much for them. No, it is actually the very last thing they need. Remember that vitamin-A without protein and or fats is a direct cytotoxin, and that is not just a “theory,” it is a fact. So, nope, sorry, contrary to popular belief, poisoning a starving kid with vitamin-A is not going to help them.
However, that is just the start of it. In India, it is hugely customary to eat rice dishes that are loaded up on hot spices and various spicy sauces. The hot spices are not just for flavoring, rather it is a survival requirement to compensate for the lack of refrigeration. Without refrigeration, it is very common for most meats being included in the rice dishes to have acquired a heavy concentration of bacteria. Thus, the spices are added as a means of killing off much of that bacteria. One of the most common, and I think it is safe to claim, the primary spice used in India is chili peppers, and chili powders. At about 30,000 IUs of vitamin A per 100 grams, that’s no small factor in the national daily intake. Then consider that sweet potatoes are common there too. Given that, for many people in India they are obviously getting tons of vitamin A into their daily diets. In addition to that information, we have a very important food preparation rule handed down over the centuries through the long chain of knowledgeable mothers. That rule is that chilies must never be combined with milk. Chilies in a meal without milk or dairy is fine. Milk and or dairy in a meal without chilies is fine. But, the two must never be combined because “it will make you very sick”. Obviously, the casein protein within the milk is acting as the carrier molecule that then transfers too much of the vitamin A from the chili across the intestinal wall.
So, how is it that vitamin-A deficiency even exists, at all, in these regions? Well, I’m here to tell you that it does not exist. On the other side of the argument, the proponents of these programs will argue that it clearly does exist. Who’s correct? Well, let’s not get into some meaningless debate about it. Rather, let’s find out. You might very logically be thinking, some simple random blood tests to measure serum levels would clear up this question rather darn quickly. Yes, you’d think so. But, remember, we are living in the negative universe here when dealing with the so-called science of vitamin-A.
Of course, those blood tests are conducted, and wouldn’t you know it, people in these regions, and even the people with the symptoms of VAD have ample amounts of vitamin-A in their serum. And, yes, that’s by our Western standards, and they have completely normal amounts of it too. Even a bit more surprisingly, the people with higher serum levels of vitamin-A have even more symptoms of VAD. I bet you are thinking I must be making this up. But no, I am not. This information comes straight from one of the premier and definitive sources on the matter:
While serum retinal levels below 20 µg/dl or in (0.7 µmol /liter) are generally considered normal there are important caveats.
- Carefully monitored vitamin-A depletion of otherwise healthy adults demonstrates impaired dark adaptation at serum vitamin-A levels between 20 µg/dl - 30 µg/dl or higher.
- Non-xerophthalmic children with serum levels above 20 µg/dl have evidence of sub clinical functional disturbances like conjunctiva metaplasia which is directly associated with other health consequences.
- A significant proportion of children with clinical xerophthalmia have serum levels above 20 µg/dl, while an even larger proportion with seemingly normal eyes have levels below 20 µg/dl.
Alfred Sommer and Keith P. West; with James A. Olson and A. Catherine Ross
Oxford University Press, 1996 ISBN: 9780195088243
Now after more than fifty years of the field work on the ground, there are a few people who are starting to question the validity and benefit of the supplementation programs. The thing is, the programs are just not working out very well. This realization was becoming somewhat obvious to front line physicians even back in the 1960s, as McLaren noted in his 1963 book.
What on earth is nutritional science good for, if, even in the atomic age, it is not capable to contract one of the foulest consequences of bad nutrition? Do you realize, that since the days of Mori, 60 years ago, not in Japan, but in countries like Indonesia, not one step forward has been taken and spite of a mountain of thoughtful attention paid by doctors?
Source: MALNUTRITION and THE EYE, forward, page ix
Even though there are now more than one hundred countries that have implemented vitamin-A supplementation programs, and we are told millions of lives have been saved, it is estimated that, globally, 190 million children under five years of age are still affected by vitamin-A deficiency.14
After more than fifty years of massive supplementation programs in these regions, the problem of VAD appears only to have gotten worse. If I understand this correctly, the more vitamin-A they distribute, the more vitamin-A deficiency they’re reporting. Even more concerning, more and more evidence is surfacing that the programs are not only not helpful, but they also are, in actuality, harming kids, and sometimes doing far worse.
Michael Latham highlights many of these concerns in his excellent analysis: The Great Vitamin-A Fiasco15
The findings that high doses of vitamin-A, especially in well-nourished children, have adverse impacts on respiratory infections, should surely be grounds for serious concern.
Journal of the World Public Health Nutrition Association
Contrary to all the best intentions and the nice sounding political messages, the facts on the ground are simply revealing the true story. Despite all the claims from the so-called Western experts, the locals are starting to wise-up to the facts and see it for what it truly is. They have been seeing it with their own eyes for decades now too. The material facts, on the ground, are that the vitamin-A supplementation programs are not only not helpful, but they are also doing exactly the opposite and are harming many kids. That fact has just become so obvious now, that the programs are being rejected by local authorities in many regions of India. They might not know why the supplements are harmful, but they do know that something is very wrong about them.
14 http://www.who.int/immunization/programmes_systems/interventions/vitamin_A/en/
15 http://wphna.org/wp-content/uploads/2014/12/WN-2010-01-01-12-45-Michael-Latham-Vitamin-A-fiasco.pdf
Actually, the bigger and far more important predicament facing many children in these regions is chronic malnutrition and not having safe drinking water. What these children really need is a reliable meal with adequate proteins and fats and clean drinking water. Somehow, the Western medical experts blindly ignore this and believe they’re helping them out by giving them a large dose of vitamin-A every year. Not only is it completely delusional to think that this is helping these kids, but it is also just beyond idiotic. Who the hell do they think they’re kidding? The only people that could be fooled into believing this nonsense is themselves. But if this idiotic practice resulted in doing no harm to health then it would be somewhat okay. It would just be a big waste of money; not a big deal. However, not only is it harming many of these kids, causing many of them to get infections and chronic diseases, it’s even killing a quite a few of them too.
With the Western medical community so absolutely convinced of vitamin-A deficiency and its endemic nature in Southeast Asia they have been supplementing kids and adults in this region for decades and decades. Yes, it has been a huge humanitarian effort funded by tens of millions of dollars per year from Western taxpayers.
And for decades and decades, there’s been a repeated little glitch randomly showing up. This little glitch is in addition to the initiation of the infectious diseases, and the autoimmune diseases, the supplementation is causing. That glitch is that some kids simply die when given a dose of vitamin-A. That’s correct, giving a vitamin supplement to younger kids sometimes kills them. Yet, very paradoxically, the younger kids are the ones in the least need of the supplementation.
The apparent absence of a protective effect before four months may reflect special circumstances of the newborn breast-fed child who will have inherited considerable immunity from its mother and obtained an additional passive immunity and vitamin-A from breastmilk. Xerophthalmia is rare among they youngest children under two years of age so presumably is moderate to severe vitamin-A deficiency.
Health, Survival, and Vision, page 38
So, firstly, is it not interesting that there’s little evidence of vitamin-A deficiency in the newborn? It just doesn’t show up, that is until the western medical doctors get involved, and start supplementing them with it.
Less clear is the reason why the youngest children (one to three months) given a large dose of vitamin-A 100,000 IU may have suffered increased mortality. Very young infants probably metabolize vitamin-A differently than older children with more mature metabolic systems.
Health, Survival, and Vision, page 38
The nonsense and unsupported rationalizations really get going here. But, clearly, they know they’re killing children by supplementing them with what’s called a “vitamin.”
Even more surprising, the apparent (but not statistically significant) excess mortality is predominantly confined to the best nourished (i.e. lease wasted) children (Fig. 2 – 14) (West KP, Kats J., Sommer A. unpublished data). The following observations are consistent with preliminary reports from one mortality trial suggesting that an apparent increase in acute lower respiratory infections is most pronounced among better nourished children receiving high-dose vitamin-A. These unexpected findings await confirmation and a biological explanation.
Health, Survival, and Vision, page 38
This statement is a remarkable, if not astonishing, display of scientific arrogance. Who the hell are they to say that it’s not “statistically significant” to be killing children? I guess it’s not “statistically significant” when it’s not their kids that are being killed.
And if they are looking for a biological explanation, it is incredibly trivially easy to see it. The better-nourished children already have ample stores in their liver’s. Therefore, the rate at which they can absorb, and safely absorb, a large vitamin-A dose is less than other children. Since it cannot be stored quickly, and without adequate fats and proteins, it is toxic. Its toxicity causes the destruction of the epithelial tissue leading to infection and maybe even blindness. So, there, done; biologically explained! Just as astonishing is their refusal to see and come to terms with reality. The reality is that it’s the perfectly healthy infants who have the lowest vitamin A stores.
The mean liver stores of vitamin A in children (1 to 10 years of age) have been reported to range from 171 to 723 μg/g (Flores and de Araujo, 1984; Mitchell et al., 1973; Money, 1978; Raica et al., 1972; Underwood et al., 1970), whereas the mean liver vitamin A stores in apparently healthy infants is lower, ranging from 0 to 320 μg/g of liver (Flores and deAraujo, 1984; Huque, 1982; Olson et al., 1979; Raica et al., 1972;Schindler et al., 1988).
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine. National Academy of Sciences.
ISBN 0-309-07279-4
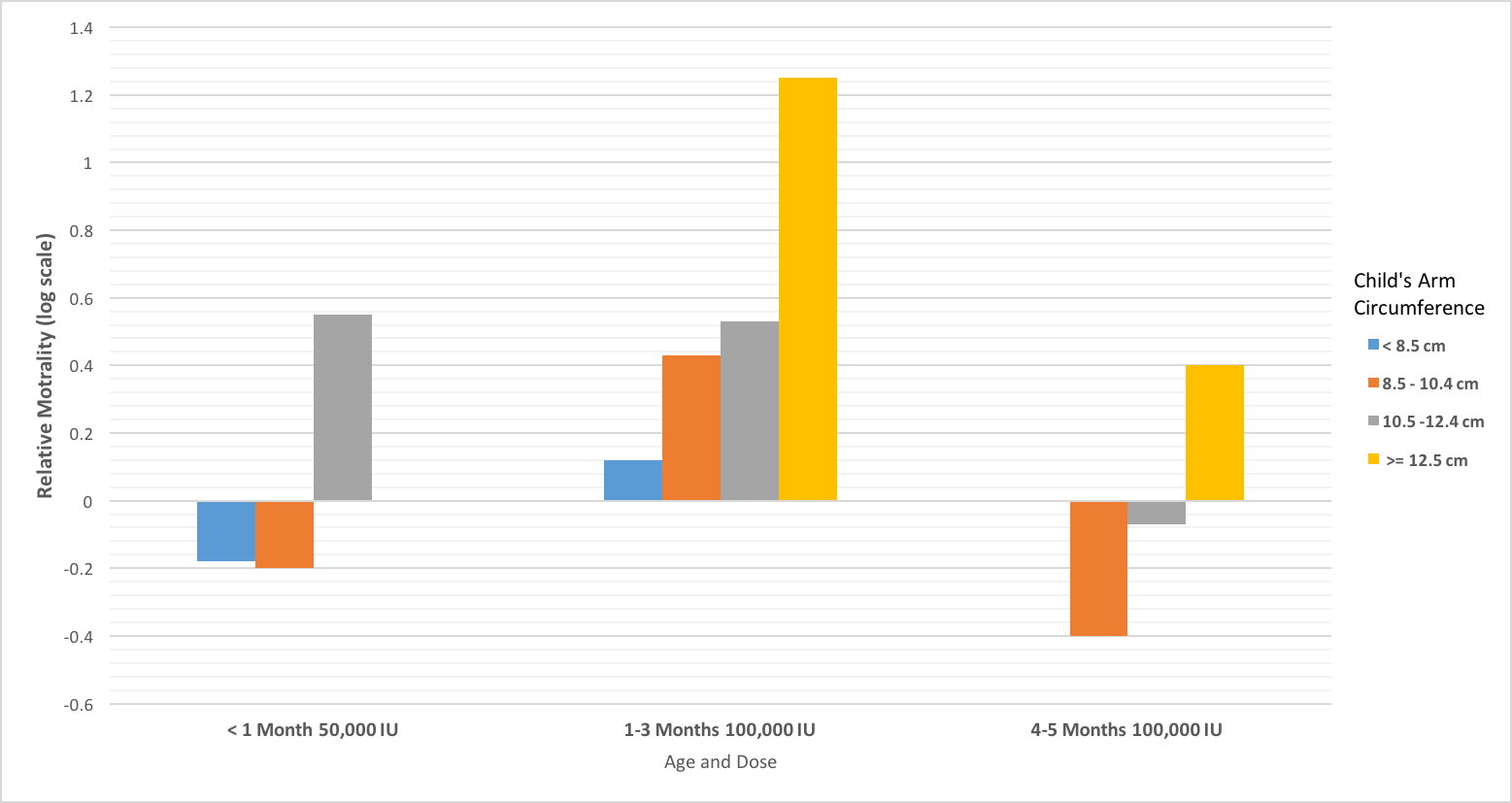
Figure 12 Relative mortality rates with vitamin-A supplementation
|
I mean, seriously, isn’t it extraordinary that healthy infants have right down to 0 μg/g of vitamin-A in their liver stores? Isn’t it just as extraordinary that these researchers don’t bother to investigate this glaring paradox?
Next, we are going to do a bit of analysis of the data summary for relative mortality rates presented in Sommer’s figure 2-14 on page 39. A very close replica of the original is shown at right (equivalent to Sommer’s figure 2-14.):
The comment in the caption includes:
Indeed, better nourished vitamin-A recipients sometimes fared less well than for placebo recipients, especially children receiving 100,000 IU vitamin-A during the second through fourth months of life.
Health, Survival, and Vision, page 39
Please note that the chart shown above is not for relative morbidity ratios, it’s for relative mortality ratios. Thus, for Sommer et al., seeing children being killed by being given a single large dose of vitamin-A is simply termed as them having “fared less well.” It’s like, Oh, no big deal, better luck next time kid. Of course, the material fact here is that these well-intentioned do-gooders are indeed killing children. The self-appointed experts rationalize away this killing as being a necessary part of the program. It’s like; yes, some of the kids must die to save the many. It’s a sacrifice we, the experts, are willing to make (with other people’s lives. It’s an old argument; “Oh, it’s for the greater good.”
But, once again, who the hell are they to think that they can go around and just randomly kill children? Nonetheless, seeing kids being killed by a vitamin, and seeing it happen over and over for decades should’ve raised some serious questions and alarms. At the very least there should’ve been a major and intensive investigation as to why and how this was happening. Don’t you think there should have been an equally intensive investigation as to why younger children are more susceptible to being killed by a single dose of a vitamin? Wouldn’t you think these experts should have been incredibly curious and very motivated to get to the bottom of that little scientific mystery?
Another little scientific mystery presented in Sommer’s figure 2-14 is why has he used a log scale on the Relative Mortality axis? Why not use a simple linear scale? Of course, you’d normally use a logarithm scale when you need to straighten out an exponential curve, or compress down a very large range of numbers. But, that’s not at all the case here. Okay, so what does that ~ log 1.22 number in the larger children in the 1-3 Months 100,000 IU group really mean? The inverse log of it is = 10^1.22 = 16.6. Therefore the relative mortality rate is more like around 17 times higher than the baseline of those kids given a placebo. Hmm… so what do you make of that? That’s right, for kids in this age group given the vitamin-A dose they are 17 times more likely to die than compared to those kids who were not given the dose. I think I can see why he was obscuring that number in the log scale.
So how many kids are being killed each year by being “given the nice vitamin-A treatment?” Well, it’s hard to know for sure since it’s not exactly a number they’re proud enough of to be publishing. But, we have some good starting information to make a reasonable approximation of it.
The potential risk must be kept in perspective: in a Nepalese population studied, high-dose supplementation of children six months an older prevented over 150 deaths for each death to which it may have contributed among younger children.
Health, Survival, and Vision, page 38
What evidence do they have that they’ve really prevented any deaths with vitamin-A supplementation? Of course, based on the new information we have, we know it’s more than likely actually zero deaths that have been prevented with vitamin-A supplementation.
But, of course, that one death out of 150 so-called saved children, does not mean that they are killing one out of the 150 children supplemented. We need to run the numbers on the ratios to get a better indication just how many children this adds up to.
It now seems clear that improving the vitamin-A status of deficient children would not only prevent 5 million to 10 million cases of xerophthalmia and a half million children from being blind each year, but save a million or more lives annually as well. In the past two years, specialized agencies of the United Nations (WHO, UNICEF, FAO) have raised their level of concern and commitment. The UNICEF Governing Board, the world health assembly, the World Summit for Children, and International Conference of Nutrition have all called for the control or elimination of vitamin-A deficiency by the year 2000.
Health, Survival, and Vision, Preface page
Other modern estimates put the number of “saved” children at about two million per year. Nonetheless, we’ll just go with the lower number for our analysis. Okay, using their estimate of more than one million lives “saved” per year, let’s estimate how many kids they are killing.
![]()
![]()
So, in each decade that’s about 70,000 kids being killed with a “vitamin” dose. Now, if anybody else were responsible for the killing of seventy thousand children, it would be called mass murder, or at least mass homicide due to criminal negligence. Yes, it is homicide; as its definition is rather damn straight forward:
Definition of homicide:
- a person who kills another
- a killing of one human being by another
Firstly, if they are going to be randomly killing some kids to save the many, then they had better be 100% absolutely, rock solidly, correct in their so-called science about it.
Secondly, with all their intervention programs, and best wishes, and stated grand goals, here we are in 2017, and the problem has only gotten worse year by year. That’s right, no matter how much vitamin-A they distribute they just can’t seem to keep ahead of the problem. What the hell is it going to take for these people to stop the bus, wake-up, and see the obvious? The programs are not only not working; they are making the situation far worse. There are now more than 100 countries in the world where the vitamin-A supplementation programs are being run. In these countries, not only is there no end in sight for the vitamin-A deficiency problem, other plagues and epidemics are now becoming common. If we just take Vietnam as an example, they have an astonishing and completely new epidemic of autism. And maybe, with the new information revealed here that so-called vitamin-A is not a vitamin at all, they’ll finally understand exactly why. Yes, ironically, they are simply poisoning and killing kids with a toxin.
One of the other very commonly cited reasons and rationales for the supplementation programs is the belief that it helps fight infections. The primary evidence for this is that it is observed when a child encounters measles their vitamin-A serum levels are dramatically reduced. From that, it is rationalized that the body is somehow using the vitamin-A to fight the infection. But, even to the medical experts, it’s perfectly clear that having ample amounts of vitamin-A does not prevent anyone from getting the measles.
Interestingly, five cases of post-measles corneal melting were observed in Leipzig Germany, in a three-month period in 1955. The authors could not explain its genesis. Although the children were generally very ill. The authors ruled out vitamin-A deficiency by the absence of any significant clinical response to vitamin-A therapy.
Health, Survival, and Vision, page 206
But, what we now know is that one of the biggest contributing factors in getting infections is compromised skin integrity and that of other epithelial tissues. Therefore, the very best way to prevent infection is maintaining strong and perfectly structured and healthy skin. The very substance proven in all the early experiments to slowly destroy these tissues is the metabolite of vitamin-A. However, just as importantly, and completely obvious to anyone who has spent any time in these countries of Southeast Asia, the greatest risk of infection is due to the dearth of proper sanitation services. There are large numbers of people living in direct daily contact with open sewage. Of course, many people have their drinking water contaminated with it too. Therefore, for the folks at the WHO still thinking that they can prevent an infection by giving the kids and adults a shot of vitamin-A, it is complete lunacy. If they really want to prevent infection, they need to assist these towns and municipalities in building the proper sanitation services and modern sewage treatment facilities. What I would like to know is, how many sewage treatment plants has the WHO built in these regions? Today, in 2017, there’s still something like 600 million people in India alone that do not even have a flush toilet to use. The situation with the vitamin-A supplementation programs supposedly helping by preventing infections in this environment is simply beyond idiotic!
But, nonetheless, there is this well-observed correlation between getting the measles, and follow-on xerophthalmia, accompanied by a drop in vitamin-A serum levels. Yet in many other cases, xerophthalmia occurs with no precipitating measles,
Typically, xerophthalmia, in the absence of precipitating measles, has been observed in most areas of Africa in which measles associated blindness occurs in which it has been sought out. Estimates that one-fourth to one-half the cases of corneal involvement are associated with measles are consistent with observations in Indonesia and reports from El Salvador Vietnam, Japan and Jordan.
Health, Survival, and Vision, page 205
Even though this information may seem rather contradictory and rather confusing, it’s very easily explained. Kids with high serum levels of vitamin-A and not having adequate amounts of protective proteins and fats will experience higher levels of retinoic acid production. In the absence of widespread infection, their dietary fats and proteins are the biggest missing factors in controlling the conversion rate.
However, the equation quickly changes when getting a large-scale infection, such as the measles. Under attack by the virus, the cell membranes are damaged or otherwise compromised, and many cells activate their retinoid receptors. Or, and far more plausibly, the cell’s damaged membranes just more easily allow the circulating retinoids to pass through.
At the same time, as part of the overall immune response, the liver is releasing large amounts of stored vitamin-A into the serum. These combined factors then promote accelerated conversion rates, leading to even larger amounts of retinoic acid being produced and released back into the serum.
The xerophthalmia problem in the countries of the Middle East has not yet been fully investigated and documented. From recent personal observations it is evident that xerophthalmia only occurs mainly in association with measles and gastroenteritis in the summer months.
Source: MALNUTRITION and THE EYE, page 222
Not surprisingly, there is another common situation that causes a large number cells to activate their retinoid receptors at the same time, and that is when people are given vaccinations.
It is now well understood that the immune system uses pathogen-associated molecule molecular patterns (PAMPs) to activate pathogen-recognition receptors such as TLR, and also a host of other more recently discovered receptors: retinoic-acid inducible gene-based (RIG)-I like receptors, or RLRs, and cytosolic nucleotide oligomerization domain (NOD)-like receptors, or NLRs. These receptors bind various pathogen ligands … more.
By Stanley A. Plotkin, MD, Walter Orenstein, MD and Paul A. Offit, MD
ISBN: 978-1-4557-0090-5
Page 59
Therefore, the more vaccinations a kid gets in one day, the greater the risk. Thus, the perfect storm scenario here is first jacking up the malnourished kids on copious quantities of vitamin-A and then giving them a bunch of vaccinations. Not too surprisingly, this is indeed the general practice when the WHO is distributing vaccines. It’s far more efficient, logistically speaking, to give kids their vitamin-A supplement and vaccines on the same day.
Yep, it’s almost perfect. We just need to expose these same kids to a highly infectious environment and lots of sunshine, and South East Asia has heaps of both of that. But, to really finish them off quickly, there are a few more hugely important and hidden variables, and they are completely unknown to the well-intentioned folks administering the vaccines. We’ll come back to this topic in a later chapter.
Regarding infections, there’s another commonly cited feature of vitamin-A magically “boosting” the immune system. But, once again the experts are failing, and completely failing, to see the obvious. Vitamin-A is not magically boosting the immune system at all. There are studies proving supplementing people of chronic diseases such as AIDS makes their situation far worse. And of course, it does. It’s because vitamin-A is damaging tissue cells. The body and immune system detect the damage to the tissue cells. The immune system then responds by building more immune cells. The body is simply responding to a toxin and its obvious threat by building the immune system bigger. In the case of AIDS, it backfires and makes the disease even worse, because having more circulating new immune cells gives the virus more opportunity to spread faster. Therefore, supplementing people in regions where there’s a high incidence rate of AIDS is going to be causing the disease to spread even faster, not just within the person, but within the community too.
In addition to this real-world evidence that vitamin-A does not help prevent or heal from infections, we have some rather interesting clinical evidence showing that it makes the immune response far less effective too.
"new evidence is emerging to show that vitamin A supplementation above and beyond normal levels may have negative health consequences. A new research report published in the July 2015 issue of the Journal of Leukocyte Biology may help to explain why too much vitamin A can be harmful. Too much vitamin A shuts down the body's trained immunity, opening the door to infections to which we would otherwise be immune. This study adds to the arguments that vitamin A supplementation should only be done with clear biological and clinical arguments. Furthermore, it also suggests that low vitamin A concentrations in certain situations may even be "normal."
Federation of American Societies for Experimental Biology
https://www.sciencedaily.com/releases/2015/06/150630121406.htm
Not too surprisingly, in this bazaar world, in the negative universe of vitamin-A deficiency science, something very strange is going on. Remember, the very definition of vitamin-A being defined as a vitamin in the first place comes from the early experiments proving that the deficiency of it caused the dreadful melting lesions seen in advanced stage xerophthalmia. So much so, that the disease and the deficiency are used nearly completely synonymously in the medical textbooks.
Xerophthalmia’s Relationship to Vitamin-A Status
As the pathognomonic clinical sign of vitamin-A deficiency, the presence and severity of xerophthalmia has classically served as a surrogate for vitamin-A status in studies investigating the relationship between vitamin-A deficiency and factors which might interact.
Source: VITAMIN-A DEFICIENCY, Health, Survival, and Vision. Page 8
However, and of course, there is now just stunning and overwhelming evidence, and it’s being presented in the hundreds of millions of people who live in North America, that this can simply no longer be the case. Likewise, the amazing contradiction is that in Southeast Asia and South America, the reality on the ground is that most people there have completely normal, and adequate amounts of vitamin-A in serum. Yet, despite these glaring material facts, the experts believe that they continue to see the symptoms of vitamin-A deficiency. Rather than seeing and facing the facts, they need to rationalize away this apparent paradox. Naturally, they fabricate bizarre and ridiculous excuses. But, even that won’t cut it. So, with absolutely no scientific basis, they are adjusting and expanding the very definition of vitamin-A deficiency to fit the narrative.
It’s not serum levels; it’s now skin lipid levels
Here’s a quote from a WHO report indicating this shift and expansion, with a newer, and very vague definition of vitamin-A deficiency.
VAD is not simply defined. WHO defines it as tissue concentrations of vitamin-A low enough to have adverse health consequences even if there is no evidence of clinical xerophthalmia. In addition to the specific signs and symptoms of xerophthalmia and the risk of irreversible blindness, non-specific symptoms include increased morbidity and mortality, poor reproductive health, increased risk of anemia, and contributions to slowed growth and development. Because these non-specific adverse consequences may occur from other nutrient deficits as well, it is difficult to attribute non-ocular symptoms specifically to VAD in the absence of biochemical measurements reflective of vitamin-A status.
You would think that the so-called experts could at least get their story straight between themselves before they publish such nonsense.
Firstly, what’s with this ridiculous, and illogical, statement that “VAD is not simply defined?” Once again, the very reason vitamin-A is defined as a vitamin in the first place is because of the consequences of the deficiency of it. If there were no consequences of the deficiency of the said vitamin, then it would not be called a vitamin at all. Without the deficiency, that was “proven” to cause xerophthalmia, and the related diseases of the eyes, vitamin-A simply would not be on the list of vitamins. Of course, the consequences of the thought to be a deficiency of it are extremely well-defined. Therefore, their statement that “VAD is not simply defined,” is not only an oxymoron, but it's also pretty much just another blatant lie.
Obviously, the other huge crack in the grand theory is now being revealed. That is, how can it be that in people with more than adequate serum levels of vitamin-A be showing signs of vitamin-A deficiency? Clearly, and logically, that’s just impossible. Therefore, the definition of VAD needs to be conveniently expanded to fill in and mask this glaring contradiction. In the statement above, the WHO is pretty much just expanding the definition to simply having low tissue concentrations. Okay, so what does “low” mean? Does anyone know?
Well, they must have missed the memo on this one too. Somehow, and mysteriously, it’s only humans that seem to need to accumulate any vitamin-A in their adipose tissues. Why is that? Maybe, it’s because rather than us humans needing it, there’s a clear message that the body is sending us here. That message is that we are simply getting too much of it, and it is leaching into, and wrongly accumulating in these adipose lipids.
But, if this “low tissue levels” excuse doesn’t cut it, they throw in a few more excuses and distractions. Things like poor reproductive health, increased anemia, and slow growth. What the heck, why stop there? Why not just blame any adverse health condition on vitamin-A deficiency?
But, once again, doing only a few minutes of research debunks these additional notions. Firstly, regarding reproductive health. The lowest rates of birth defects are seen in women with the lowest serum levels of vitamin-A. That’s correct, odd as it may seem, women with an incredibly poor vitamin-A status give birth to anatomically perfect babies.
It has been suggested by Millen and Woollam (1958) that the teratogenic effects of hypervitaminosis A may be brought about by inducing a deficiency of vitamins of the B complex, for adding these vitamins prevented the malformations due to excess vitamin-A. Similarly, a general deficiency of protein or starvation do not appear to have teratogenic effects.
Whereas, it’s the complete opposite happening here in North America. We now have some of the highest rates of birth defects in the world, right along with our highest vitamin-A serum and tissue levels.
Next, let’s address this concern about anemia. What’s truely happening is that as cells are over exposed to retinol, they produce retinoic acid. That retinoic acid needs to be quickly buffered with calcium. The body draws calcium from the bones. Calcium combines with oxygen and iron to form and undergo a natural exothermic reaction. That reaction then causes inflammation. That reaction thus consumes considerable amounts of the iron from the blood. The low iron levels in blood then lead to its low oxygen content and then subsequently to downstream ischemic damage. And, let’s not forget that to have iron in the blood in the first place, you need to have a source of it too. That usually comes from eating red meats.
Finally, to address their last point about slow growth, let’s consider Kenya. Kenya is reported to have one of the worst, and endemic, vitamin-A deficiency rates in the world. It’s currently reported to be at a rate of about 85% of the population. Paradoxically, Kenya produces some of the tallest people in the world. A well-documented biological measure of overall human health is how tall people grow. Additionally, if the experts from the WHO haven’t noticed it, many of the top Olympic sprinters and runners are from Kenya. Therefore, somehow to the experts, observing: tall, fast, healthy people, hmm, this is not normal, it must be endemic VAD.
I think it’s rather clear to see that their conveniently broader definition of vitamin-A deficiency is complete, utter nonsense and has no basis in reality, or in science. It’s even more convenient that there are no “reliable biochemical measurements reflective of vitamin-A status.” In other words, they’re just wholly fabricating this new broader definition.
Now, running large multinational vitamin-A supplementation programs using capsules is a rather big logistical problem. You need to employ a very large number people on the ground actively distributing and dispensing the capsules. Therefore, the funding needed for these programs is probably in the order of tens, or maybe even hundreds, of millions of dollars per year. Additionally, it would be very difficult to keep track of the people, both kids and adults, who have been given the supplementation and those that haven’t. Furthermore, the capsule programs might be a bit risky because some people could easily be dosed twice or more in one program cycle. On the flipside, the coverage would be rather sporadic and spotty too. Naturally, the programs need to be run perpetually, year after year, too. Overall this is a huge, industrial-scale, logistical problem. Therefore, the WHO has taken an industrial scale approach to solving it. In addition to the capsule programs, they have been widely supplementing both Sugar and MSG with vitamin-A. Reading Sommer’s perspective on this, he’s quite proud of the accomplishment of getting vitamin-A manufactured into sugar and MSG.
However, even before knowing that vitamin-A is not a vitamin, this goes way beyond foolishness, it is simply insanity. With vitamin-A being added to these staple food products, and having no control whatsoever who gets it and how much of it, they’ve set the stage for a catastrophe on an epic scale. It won’t be just in the sugar and MSG that people buy directly in packages; it’ll be hidden in the sugar and MSG that’s included in so many of the processed and prepared foods of the region. It will even be hidden in soft drinks. The people of these regions will have no idea of the long-term risks.
However, what the folks at the WHO do know, and they know it with absolute certainty, is that vitamin-A is a fat-soluble molecule. They do know that over time it will accumulate and eventually people will get to a toxic state with it. They do know that once people get to a toxic state with it that they will become horribly diseased. They do know that there is no known antidote. Therefore, they are poisoning the major populations of the Southern Hemisphere, and they have no backup plan for getting people out of it.
Not to be dissuaded by those little scientific facts, they remain totally committed to maintaining the supplementation programs. They are so focused on some perceived short-term gain, that they are completely ignoring the certain long-term pain. Their programs are simply a deal with the devil. When I first read about the addition of vitamin-A to sugar and MSG, I could almost not believe it. Supplementing sugar with vitamin-A is like the perfect, and the absolutely perfect, drug to induce obesity combined with diabetes in people; and do it on a near worldwide scale too. Now, is it any wonder why the world is facing an emerging diabetes pandemic? It’s a pandemic that has diseased at least 350 million people, and is currently killing about 6 million people per year too.
The immediate question I asked, is this even legal? Do the people in these regions being supplemented with vitamin-A via sugar and MSG even realize that it’s there? If they don’t, then they might not limit the consumption of it at all. Moreover, what we already know is that for the vast majority of these people they are actually already getting more than ample amounts of vitamin-A from their regular diets too. Therefore, these new food-based supplementation programs perpetually add more of it, and will accelerate them into a disease state. Even if the people of these regions did realize the supplemented vitamin-A was hidden in their sugar and MSG, most of them would have no idea about the long-term risks and potentially devastating consequences of it.
It’s an experiment, at best. Is it legal to experiment on large-scale human populations without their informed consent and their full knowledge of the risks? No, it is not. It is a crime. So now, here we have doctors, who are knowingly killing thousands of children under the guise of it being for the greater good, and they are also committing the same offense for which the Nazi doctors were tried for at Nuremberg after the Second World War.
1. The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion, and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject, there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment. The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs, or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.
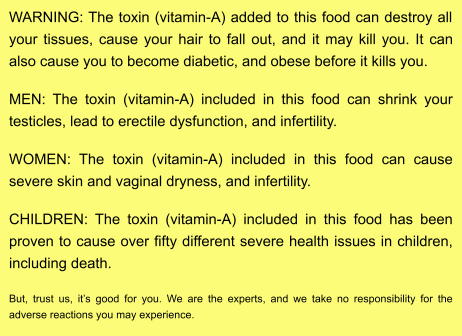
Proposed food label for vitamin A supplemented SUGAR and MSG
|
At best, the vitamin-A supplementation programs are botched experiments that violate this code. Since it has been conducted on a worldwide scale, and it has now knowingly killed tens of thousands of kids and has very likely made millions of people sick and diseased, it should be regarded as a crime against humanity. Governments secretly and deceitfully deciding on their own to conduct this experiment on all of us is a crime. But, at least we now know. They have revealed their hand.
In the spirit of openness and honesty (and even before knowing that vitamin-A is not a vitamin), here’s a proposed food label for vitamin A supplemented SUGAR and MSG being sold in the regions.
Now, to all the proponents and advocates of the VA supplementation programs, I have some shocking new information for you. VAD has never been proven in animals nor in humans, not ever, not even once! The very foundation of the vitamin-A deficiency theory is absolutely and completely junk science, and it is simply wrong. The VAD theory is very likely nothing more than corrupt science perpetrated by con artists. The emperor has no clothes. Thus, with that new knowledge, can you please now stop poisoning and killing the children with it.
From the early vitamin-A deficiency experiments it was clear that there was a catastrophic effect on the reproductive organs for both males and females. But, we now know these experiments weren’t proving the deficiency at all. Rather, they were really proving the toxicity of the vitamin-A metabolite, that of retinoic acid. Since the vitamin-A supplementation programs have been conducted in Southeast Asia for over four decades now, there has been ample time for us to start seeing the consequences of that in terms of fertility rates. Clearly, some of that supplemented and accumulated, vitamin-A will have been slowly converting into retinoic acid.
Of course, the supplementation programs are not just limited to Southeast Asia and South America. For us here living in the West, we too have had it supplemented to most of our low-fat dairy products, margarine, and many other foods since the 1970s. Therefore, it should be rather interesting to look at what’s been happening to the worldwide human fertility rates over the last four or five decades. And sure enough, there has been a dramatic drop in the human fertility rates in Southeast Asia, South America, and in North America too, since the supplementation programs were implemented.
Naturally, one question that’s probably coming to mind is; Is this just botched science or has it been made to happen? Although I firmly believe that it is indeed just botched science, the scale and magnitude of the consequences of it are almost unbelievable. Yet, there’s a middle ground scenario that needs to be considered. That is, is this then botched science that someone has decided to take advantage of and allow it to silently continue? I have no idea about that, but I think it should be investigated.
In the previous chapter, I mentioned the Nüremberg Code of medical conduct being applied to Nazi doctors after the Second World War. Naturally, for anyone to talk about grand conspiracy theories, there usually needs to be some tie-in with the Nazis. Firstly, if you’re not aware of it, the senior people and commanders running the Nazi death camps were mostly doctors. That’s correct, what should’ve been medical healers had been turned into medical killers, and they killed on a massive scale. In addition to their mass killing agenda, the Nazi state had an equally important prime and sinister objective of being able to induce mass sterility in the human population. Their goal with this agenda was, of course, to be able to keep a large human slave labor workforce and do it on a worldwide scale. To achieve this grand goal, they needed to ensure that their slaves couldn’t and wouldn’t reproduce unless their Nazi masters allowed it. The research needed to achieve this goal was viewed by Himmler and his associates as being the highest priority “agricultural project.” For them, their human slaves were viewed as being nothing more than a herd of animals, and that herd needed to be managed as such. It was an essential part of the giant farming operations that would be needed to feed the Third Reich.
There is a very thorough investigation, along with its deeply disturbing revelations, into the thinking and the genocidal psychology driving these doctors in the book titled: THE NAZI DOCTORS, Medical Killing and the Psychology of Genocide by Robert Jay Lifton, published in 1986.
The Nazi doctors had investigated several approaches for massive sterilization. There were several investigations with injecting prisoners with various sterilization toxins. Although the injections proved to be somewhat effective, there was no way they were going to scale up to administer this procedure to be applied on a worldwide basis. Therefore, they went looking for chemical solutions they could add to food. One of the more prominent Nazi doctors who headed up these research projects was Carl Clauberg. Clauberg worked directly in his own research facility within the infamous Auschwitz camp. His work was beginning to show real promise as the war was coming to an end. The allies had captured the camps, and Carl Clauberg was taken prisoner by the Russians. Then in 1955, in a prisoner exchange with the American administrators of post-War Germany, Carl Clauberg was returned to Germany. Rather astonishingly, after having perhaps killed thousands of people, and sterilizing thousands of young women, Carl Clauberg simply goes back into medical practice as a doctor. After his repatriation back to Germany, he’s not only unrepentant but proudly acknowledges his participation and achievements at Königshütte Auschwitz.
When interviewed by the press, he spoke proudly of this work at at Königshütte and Auschwitz and claimed, “I was able to perfect an absolutely new method of sterilization… Which would be of great use today in certain cases.”
Source: The NAZI Doctors, page 277
Likewise, for many of the other doctors who were involved with and worked in the Nazi death camps, they were never put on trial after the war. They simply went home, put away their rifles, hung up their uniforms and put on the white lab coats. And like with Carl Clauberg, for many of them their ideology wasn’t changed, and the mission hadn’t changed one bit either. It was the same people, the same ideology; it was just new tactics that needed to be adopted. Rather than using bullets, and gas chambers, they picked up their syringes and their newly found special toxic molecules and went straight back to work. Although I am somewhat speculating on this, there’s a good bit of evidence to support this claim that some of these doctors did indeed bring their death camp discoveries into post-war commercial use. A good example is documented in the BBC film by Harold Evans regarding the origins of thalidomide. It is titled: Attacking the Devil: and the Last Nazi War Crime. However, that Nazi invented thalidomide and it subsequent use post-war as a commercial drug given to pregnant women may not be their last crime.
Do you think that with all those Nazi doctors running the death camps, none of them, not even one of them ever noticed that their prisoners were not developing xerophthalmia? Do you think those top doctors, with their fine German educations were not very aware, and fully expecting their prisoners to quickly succumb to the horrible conditions of vitamin-A deficiency? Don’t you think they were not a little surprised when it never appeared, like almost not at all, even in hundreds of thousands of prisoners?
Likewise, the same goes for the P.O.W. camps. Do you think, for one minute, that the astute and very well-trained Nazi doctors did not notice the complete lack of vitamin-A deficiency symptoms showing up in the large prisoner populations they held in these camps? These camps held tens of thousands of prisoners. The overall P.O.W. population was in the millions.
The very discovery of vitamin-A and its dreadful deficiency consequences would have been a rather extraordinary medical story in this era. Meaning, for many people in the medical sciences the topic of vitamin-A deficiency would have been somewhat fresh on their minds. Moreover, for a zealot like Carl Clauberg, he would’ve been scouring every bit of medical research that even remotely mentioned infertility or mentioned any chemical that had any negative influence on the reproductive organs. Do you think for one second he didn’t come across the vitamin-A deficiency research and not find it very intriguing? Additionally, for anyone with any farm experience, or any experience with animals in nature, he would’ve immediately known just how stupid the conclusions of these experiments were. Just imagine Clauberg sitting there one morning, in say the spring of 1944, and reading this so-called medical research on vitamin-A deficiency. He carefully reads about the disintegrating epitheliums, with the corresponding blistering lesions of the skin and eyes, the melting corneas, the failing organs, epileptic seizures, paralysis, and most of all sterility. He’s in complete disbelief that all of this is being induced in just eight weeks of the deficiency. He then turns and looks out his window at the great mass of people lined up for the daily morning counts. He scrutinizes the faces; the skin is clear; the eyes are big and white. He picks up his binoculars for an even closer look. He focuses right in on the faces, and carefully examines them. There are no lesions, none whatsoever. He looks back at the research paper, reads more details of the catastrophic and body-wide destruction induced in the experimental animals. He then again turns and looks out his window, and right there in front of him he sees 5,000 people who have persisted on a starvation diet, and under slave labor conditions and not a speck of hygiene, for years and not one of them, not a single one of them, shows any signs of these symptoms.
| Inactivated* technical casein (Merck) Corn-starch Cottonseed oil Salt mixture, McCollum No. 185 (6) Vegex (lVIarmite) (for vitamin B) Decitrated lemon juice (for vitamin C) Distilled water |
20 gm. 50 gm. 15 gm. 5 gm. 5 gm. 5 cc. 50 cc. |
|
|
* By heating and aeration (Goldblatt and Morltz (5)). |
||
Clauberg then turns back to the American research paper and starts to run his finger down the list of ingredients making up the diets being fed to the rats. His finger stops on this one particular line:
He’s found it! He then slowly forms the utmost sinister ear to ear grin. He picks up the phone and calls an associate at Merck, and says: “I need to know all the details of how you guys are deactivating the casein with heat an air.”
Here is a hypothetical follow-on watercooler conversation between Clauberg and one of his top assistants, say a Nazi chemist named Dr. Johannes Goebel, at the ye old death camp administration office.
Goebel: Dr. Clauberg, haven’t you noticed that our prisoners are not getting sick or dying from vitamin-A deficiency? We’ve had hundreds of thousands of them in captivity for years. We feed them nothing but dirty water with a mere pinch of barley a day. After years, their skin and eyes remain perfect. We’ve worked them non-stop as slaves, yet none of them have organ failure. None of them have any signs of vitamin-A deficiency whatsoever. It’s not to be seen in any of them, not even in the women or the children. How can that be?
Clauberg: Of course, I’ve noticed that. Obviously, the American researchers blew it. Their vitamin-A theory is nonsense. Those Ivy League school boys probably didn’t even know what end of the rat to feed.
Goebel: But if that’s true, then what was poisoning the animals of their experiments?
Clauberg: Oh, I have found exactly what it was, and it is perfect. I’ve been testing it in my lab. In the men, it first inflames and swells their testicles; then it causes their testicles to slowly shrivel and become completely atrophied and dysfunctional. It perfectly sterilizes them. It’s equally effective on women; it dries them out and destroys their ovaries and other reproductive tissues. It’s absolutely perfect. It dumbs people down, makes them fat and weak, makes them fearful, and keeps them completely infertile. Herr Himmler will be thrilled!
Goebel: But, Dr. Clauberg, if that’s true, should we not warn the American doctors?
Clauberg shouts: No! You doofus, of course not. It is precisely what we’ve been searching for. This must be kept top-secret. Besides, they are now our enemy, if we should lose this stage of the war, we will sell them even more of their wonderful vitamins. It will slowly cause them to all get sick and die. We’ll eventually win the war, even long after they think it’s ended.
Okay, obviously, all that above is a rather fanciful bit of fictional conspiracy theory on my part. Next, let’s look at some data representing what’s happening in the real world with human fertility rates since the end of the second world war.
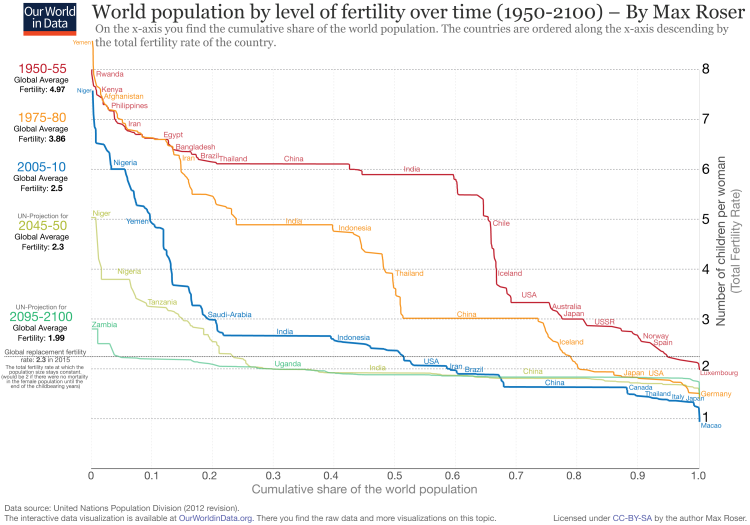
World population by level of fertility
Source: Max Roser (2016) – ‘Fertility’. Published online at OurWorldInData.org. Retrieved from: https://ourworldindata.org/fertility [Online Resource] |
An excellent resource for this data is the site by Max Roser, https://ourworldindata.org/fertility.
Obviously, for any species to be viable, it must be able to maintain the reproductive rate of at least 2.0. If that’s not the case, that species will quickly face extinction. Looking at the charts presented by Max Roser, humans could be facing extinction around the year 2100. On the geologic timeline, or in the evolutionary sense, that drop in the fertility a rate from around 7 down to less than 2 will have happened in the mere blink of an eye. Therefore, I think we need to get an exceedingly clear understanding of what’s truly going on here with global human fertility rates.
Overall, the data and resources presented on the Our World in Data website are excellent. However, the rationale used to explain this phenomenon of rapidly dropping reproductive rates is that as the human economic conditions improve the perceived need for producing more children is decreased. The belief is that people no longer think they need more children because of their own chances of survival, and that of their offspring is so much higher. So basically, the theory is that it is now it is simply a lifestyle choice to have less than two children. That’s a nice theory, and of course, the same narrative is viewed and repeated by many other researchers and experts. Except, it is not consistent with the laws of nature and biology. Biologically, we all should have an inbuilt need to reproduce as much is possible. Secondly, in the human experience, it used to be rather fun to make babies. Additionally, with the improved economic situations, people should feel a lot more confident that they can have more children and yet adequately feed them and raise them into being healthy adults. Of course, there’s an incredibly important difference between reproductive rates and fertility rates.
The most cogent bit of evidence we can apply here to debunk this overall “it’s a lifestyle choice” theory is what’s happening in North America. Here, on the one hand, we have the best economic situation in the world, at least we believe that to be true, and we have birth control, and the reproductive rates for the natural North Americans (not newly immigrated populations) have indeed fallen well below 2.0.
Number of Births | Birth Rates
|
So, that data fits with the economic theory. But, on the other hand, the material fact is that every single city in North America has infertility clinics, and most with long waiting lists, trying to help young couples get pregnant. How can that need be possible? Here we are living in the most well-nourished, well medicated, safest conditions in the world, and we have this huge infertility problem. Moreover, look what happened in North America in the period from 1955 through to about 1965, it was the Baby Boom. The economy was booming, young couples were “booming” and the babies followed. People were generally optimistic and positive about their futures and then they had more babies. Therefore, that’s a huge amount of evidence that almost by itself completely debunks the theory that the big drop in fertility rates is due to better economic conditions. Now, the fertility rates have made a big U-turn from their 1960 highs, and with a steady decline have sunk well below 2.0 in North America. Once again, how can that be possible?
Now, in the USA the fertility rates have dropped to record lows, and to below replacement levels.
“Yes, it’s below replacement level, but not dramatically so,” Dr. Brady said. “We have a high level of influx of immigrants that compensates for it.”
Source: https://www.nytimes.com/2017/07/03/health/united-states-fertility-rate.html
Here’s the same pattern of thinking that I’ve seen displayed over and over by medical professionals. In the face of the glaring and obvious facts that North America (as a society) is now profoundly sick, they fabricate these bizarre and ridiculous excuses to try to minimize it or rationalize it away. Here, in this example, they hope that we are all so gullible enough to believe that having our young couples too sick and infertile to maintain the nation’s population is somehow acceptable because we can just make it up with more immigration. Of course, it is not at all acceptable, and it’s completely the opposite. Rather, the situation should be regarded as a national disaster that will eventually erode the social fabric and self-identity of our nations. And, covering up this appalling infertility reality with more immigration is like putting a band-aid on the toe of a patient with a brain tumor. Of course, what they don’t want you to know is how and why the most fundamental biological process in our young people has now become so gravely compromised.
Annual average growth rate, natural increase and migratory increase
|
Here’s what’s going on with fertility rates in Canada:
Infertility among women age 20-to-34 increased from 9% in 1994 to 20% in 2010. Therefore, within just 16 years, our national infertility rate has more than doubled. Accordingly, we too are basically backfilling the loss in our reproductive rates with more immigration. Very peculiarly, new immigrants don’t seem to have an infertility problem. It only seems to show up in their second generations (as do their autoimmune diseases). Clearly then, there are some subtle underlying health conditions that are causing it to happen. Obviously, infertility is a caused health condition, and not the result of an economic condition, or lifestyle choice.
The second most cogent bit of evidence that we have in debunking the “it’s a lifestyle choice” theory, is that North American couples are facing at least three other silent epidemics regarding their reproductive health. That is an epidemic of vaginal atrophy and dryness,16 erectile dysfunction, and about a 50% drop in sperm count for men compared to that of the 1970s.17 Clearly, these health conditions are not lifestyle choices. But, they are indeed all symptoms of insidious vitamin-A toxicity. Don’t you just think, that just maybe, … there’s a connection here? And, since it is also the exact same toxic chemical that’s been legislated into our staple foods since the 1970s too, it just can’t get to be more straight forward than that. Yes, the top brilliant geniuses of science, the medical experts, have poisoned the reproductive health of at least half of the human population!
Now, do I believe that this is a deliberate reincarnation of the Nazi’s global sterilization agenda? No, I do not. Not for one minute. What I firmly believe is that the very foundation and basis for this problem lies in botched science. However, what did happen during the Second World War is a lesson that we can never forget. That lesson is that evil does exist and will rise up whenever it’s given an opportunity (and more so when there’s a huge profit to be made). Therefore, we need to be forever vigilant and on guard. We should pay heed to this rather disturbing warning from Robert Jay Lifton,
Totalism in the nation state, then is most likely to emerge as a cure for a death-haunted “illness”: and victimization, violence, and genocide are potential aspects of that cure.
Source: THE NAZI DOCTORS, Medical Killing and the Psychology of Genocide by Robert Jay Lifton, published in 1986. Page: 473
It was the fear of disease that the NAZI’s used to seed and fuel the national hatred toward the Jews. They used this same fear to rationalize and justify the rounding up of children with schizophrenia, or other psychiatric disorders, and then having them secretly and systematically executed by their medical establishment. Likewise, today the pharmaceutical industry has terrorized the population with the fear of infectious diseases and cancers to solidify their market positions. But, when you really analyze it, the greatest infectious parasite inflicting disease and destruction on our nations is the pharmaceutical industry itself. If that statement comes across as nasty and harsh, I’m sorry, it is just the truth, and it needs to be openly talked about.
16 Vaginal Atrophy: The 21st Century Health Issue Affecting Quality of Life
http://www.medscape.org/viewarticle/561934
17 http://www.npr.org/2017/07/31/539517210/sperm-counts-plummet-in-western-men-study-finds
Okay, by now we should have done some serious damage to the entire theory of vitamin-A deficiency. I would like to think we’ve torpedoed it enough times, and from enough angles, that it’s a burning hulk sitting dead in the water. I’d hope that the very definition and categorization of retinol being a “vitamin” is in danger of sinking below the waves of scientific history. Even though I am optimistic about that, I am not naïvely thinking that it is going to happen anytime soon. The Vitamin-A proponents will come scrambling to its defense and will do anything to keep that from happening. One of the heavyweight countermeasures to this attack will be the claim that the vitamin-A deficiency theory is proven in the hard, and exact science of chemistry. They will claim that there is rock solid scientific evidence, established by expert Ph.D.’s, showing retinal in the rhodopsin of retina of the eye and that the very process of vision is a chemical reaction that continuously consumes this form of vitamin-A. They might reasonably say something like: “Oh, you’re such a foolish little man, the case is completely closed, there’s no chance in hell you, or anyone else, can refute it!” Basically, the story is:
Vitamin-A is an essential component of vision. Light-receptor visual cells called “rods” in the retina of the eye enable us to distinguish between light and dark. These cells contain a light sensitive pigment called rhodopsin, which is a complex of the protein opsin and vitamin-A. When a rod cell’s rhodopsin disintegrates, releasing electrical charges to the brain. This reaction results in vision. During the reactions in the retina, some of the vitamin-A is lost and replaced from blood.
(Sarasota, FL: First Edition Publishing, 2013),
ISBN: 978-1622872-66-4; Page 59
|
Table 3 Attributes of human vision |
||
| Attribute | Value | |
| Pixel resolution per eye | 567,000,000 | |
| Images sampled per second | 60 | |
| Number of eyes | 2 | |
| Seconds in 16 hours | 57,600 | |
Well, on the surface of it, it’s a nice sounding theory. But, I think you’ll quickly see how completely absurd it truly is. Let’s run the numbers and do a basic sanity check on it. Here are some interesting ballpark figures about vision in the human eye.
Therefore, in each, and every, 16-hour day, the eyes would be processing about 3,919,104,000,000,000 chemical reactions. Hopefully, that looks like a pretty darn big number to you. However, that’s not just a very large number of chemical reactions; these are exothermic reactions to boot. If we had this number of heat-generating chemical reactions occurring in the eyes, each and every day, it would completely cook the eyeballs in place. The second sanity-check question to ask is what happens to all the reaction byproducts? Where does it all magically disappear to? Would it not fill-up the eyeball with gunk, as it cooked them? The lovely vitreous humor18 might not remain too vitreous for very long. At the very least, wouldn’t having a bunch of reaction byproducts accumulating in the eye obstruct light transfer? Next, depending upon how many retinal molecules are used up in each supposed-reaction, the amount of retinal needed to resupply the eye each day, would very likely surpass the human lethal dose. Not only that, according to the vitamin-A theory, the amount of retinol needed by the eye, is minuscule compared to the overall body requirements. Therefore, the required daily consumption would kill a kid within the first few days of opening their eyes. Do you really think nature would be this foolish? However, the logical flaws don’t stop there. The other well-known little fact is that the photodecomposition of retinol/retinal results in byproducts of the reaction that are extremely toxic and cancer causing agents.
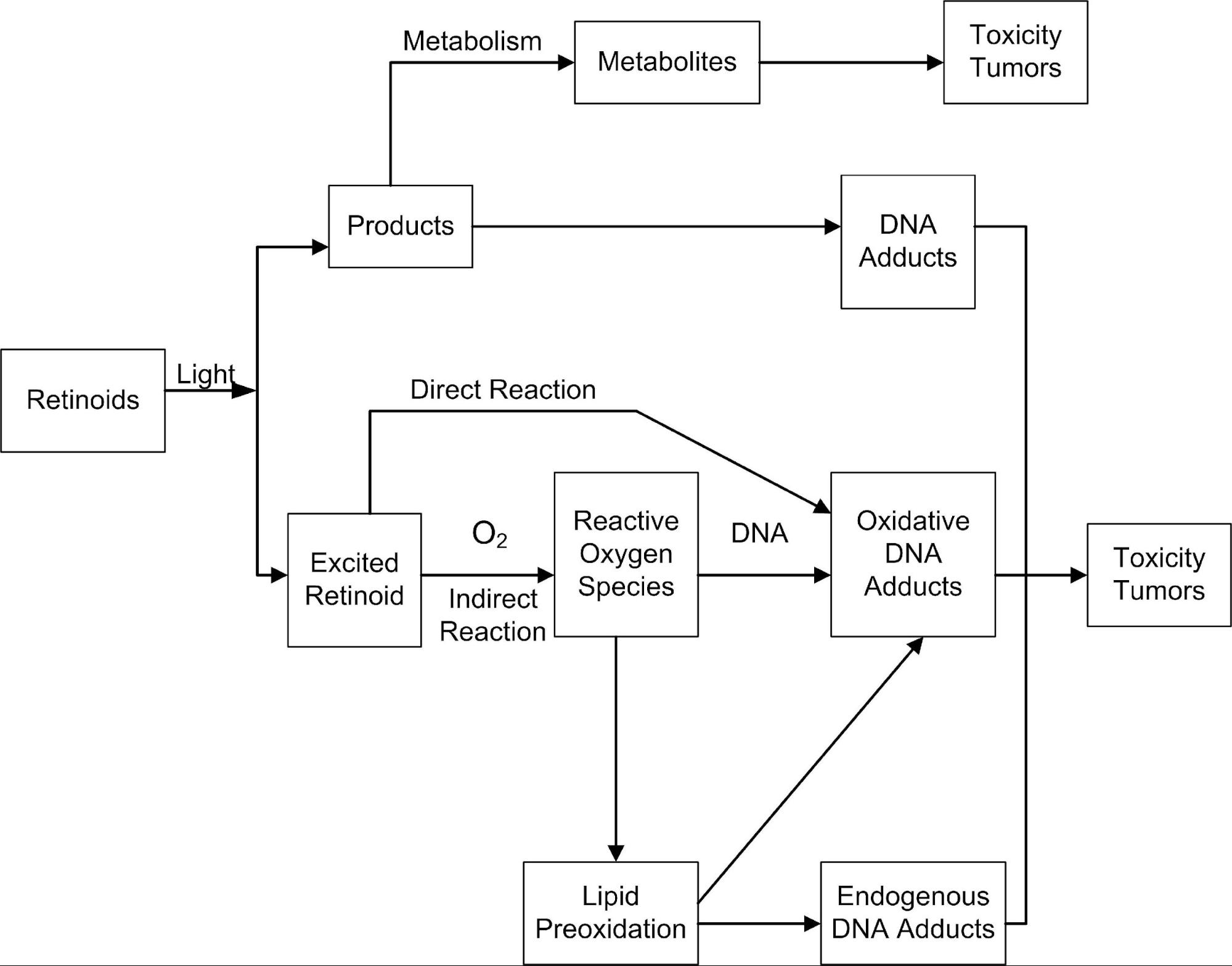
Figure 13 Photodecomposition and Phototoxicity of Natural Retinoids
Source: Figure 8: (replica) Potential photoreaction pathways of retinoids leading to phototoxicity and tumor formation Tolleson WH, Cherng S-H, Xia Q, et al. International Journal of Environmental Research and Public Health. 2005;2(1):147-155. |
Figure 13 is from the 2005 report titled: Photodecomposition and Phototoxicity of Natural Retinoids.
Overall, this is an excellent report, and it highlights the complexity of the interactions of the various retinoids and their photodecomposition carcinogenic byproducts.
Perspective
Regarding human toxicity, the long-term consequences of using cosmetics containing RP are currently unknown. It has been demonstrated that photoirradiation of RP can result in forming toxic photodecomposition products, generate ROS, induce lipid peroxidation, and cause DNA damage. Also, topically applied RP produces many of the cutaneous changes associated with the use of drug products containing RA which in some instances can enhance photocarcinogenesis.
Therefore, in addition to that nice vision as a chemical reaction cooking the eyes, and requiring us to consume daily lethal quantities of the needed retinol, the photodecomposition byproducts will surely and quickly cause eye cancers too. Once, again, do you really think nature would be this foolish? You might not, but there are many experts in the medical sciences that do.
Retinal is the vitamin A derivative that is most toxic, due to its chemical reactivity. Even when vitamin A is used only for light sensing, retinal can be toxic [119] due to its chemical toxicity in randomly modifying proteins through Schiff base formation.
Ming Zhong, Riki Kawaguchi, Miki Kassai and Hui Sun*
Nutrients 2012, 4, 2069-2096; doi:10.3390/nu4122069
Department of Physiology, Jules Stein Eye Institute, and Howard Hughes Medical Institute, David Geffen School of Medicine, University of California, Los Angeles, CA 90095, USA;
And just a bit later they state:
Although human vision in a sense perfectly serves our daily needs, we are living with the consequences of the choice of monostable pigments in evolution. If this choice helped our ancestors survive at night, it came at a surprisingly high costs. It is astonishing to realize that every photon we see depends on a complex enzymatic cycle that consumes cellular energy and releases free toxic retinoid. As we see using our cones in natural daylight or artificial light, a staggering amount of energy is consumed, and a constant flux of toxic free retinoid is cycling between cells to regenerate rhodopsin, which plays no role in daylight vision. In a sense, a whole range of human diseases, from our vision’s high sensitivity to vitamin A deficiency to Stargardt macular dystrophy, are the price we pay for this evolutionary choice.
Source: as above, page 2085
What’s so astonishing is that they continue to believe that every newborn child is immediately starting to poison themselves by simply opening their eyes to see the world around them. The experts think it’s with the powerful toxin byproducts of the nasty chemical reaction needed to fuel vision. They state that every photon entering the eye causes this toxin producing chemical reaction. Thus, they believe that nature has made this colossal design mistake. But, at least they are acknowledging that retinal, and its toxic chemical reaction byproducts, is causing a “whole range of human diseases.” Additionally, they are stating that since rhodopsin has no role in daylight vision, nature has made this extremely foolish choice of facilitating nighttime vision, at the price of our long term evolutionary survival. However, nature is no fool. Rather, it is the experts who have been fooled. Of course, this concept of vision being a very complicated chemical reaction that occurs at the speed of light simply violates the laws of physics. It is a chemist's fabricated view of the vision process, and it is clearly wrong.
18 the transparent jellylike tissue filling the eyeball behind the lens
The next major logical flaw in the vision as a chemical reaction theory is that it in no way explains color detection. The human eye can distinguish about 10,000,000 different colors. Therefore, in addition to the 3,919,104,000,000,000 chemical reactions going on in the eyes per day, they all need to be somehow variable in 10,000,000 different degrees or graduations. How do you get an instantaneous chemical reaction to be precisely variable in 10,000,000 separate increments? How do you get it to happen exactly, and precisely the same, and day after day, and for an entire lifetime too? Umm… the answer is that you don’t. I hope by now you are not buying this vision as a chemical reaction fairytale.
The next significant logical flaw in the theory is how do they explain vision to be so uniform not only from day to day but from morning till night too? Surely, with the 3,919,104,000,000,000 chemical reactions going on per day, you’d quickly locally deplete the supply of retinal within the retina. Logically thinking, that would then lead to extremely blurred, and fast fading vision as the day progressed. This condition would also happen randomly throughout the day and even vary between meals. In the mornings, your vision might be extra bright, but any drop in retinal resupply would adversely affect the vision during the day. This process would be very analogous to the sluggish feeling due to dehydration or a serious drop in blood sugars. You’d also expect weird things occurring, such as color vision fading to black and white. If the retinal supply were to be interrupted, even for a few seconds, and drop too low, you’d experience times of complete blindness too. Therefore, in nature, almost all animal species would have quickly succumbed to this flaw, and have been taken out of their evolutionary existence.
Of course, this never happens. It does not even happen in times of complete and prolonged starvation. It does not happen in animals, and it does not happen in humans. It is completely absurd for this to happen. Moreover, we’ve learned above that it has been proven not to happen, and proven not to have happened hundreds of thousands of times over when people are chronically starved for three or more years.
It has also never happened to me either. As much as humanly possible, I’ve tried to not consume a single molecule of retinol, retinal, or any of the carotenoids for nearly three years now. It’s reported:
The percentage of total body vitamin A stores lost per day was approximately 0.5 percent in adults consuming a vitamin A free diet.
Sauberlich et al., 1974
Therefore, at that rate, after about 200 days, I should have had nearly entirely depleted my body’s store of vitamin A. Yet, I’ve now gone past 1,000 days, so that’s five times as long. Therefore, I should be totally blind. Yet, my vision has only improved and remains excellent. Here’s something you may find amusing. I cycle commute to work each day, and I wear dark sunglasses. The sunglasses are mostly to keep the wind and dust out of my eyes, but also, of course, to deal with the morning sunlight too. In our winter months, it is dark when I cycle back home. I wear the same sunglasses at night. I even cycle through a large park with no street lights. That’s right, I ride my bike at night, in the dark, wearing sunglasses. Not only do I have no sign whatsoever of night blindness, but I can also see very well at night in this very low light condition. I have no problem with photo reception after nearly three years of being on a diet completely void of retinol, retinal, and its precursors.
Hopefully, with all of that, it should be very clear that there is not a chance in hell of the “vision as a chemical reaction” theory being correct.
What’s astonishing about the “vision as a chemical reaction” theory is that it is completely illogically extrapolated to the other tissues of the eye. By finding retinal in the rhodopsin pigment in the rods of the retina, it was like: “Ah ha! We’ve found the clincher in the vitamin-A deficiency case, it’s retinal.” But, the truth is that, and by a huge factor, the so-called vitamin-A deficiency diseases of the eye predominantly manifest in the other tissues of the eye, and not in the retina. These other tissues have no connection whatsoever with the image processing function of the retina, and no need for retinal, at all. There is no rhodopsin or even vitamin-A normally found in these tissues. To make the point perfectly clear, let’s consider the lens of the eye. The catastrophic end stage of xerophthalmia is the disintegration and piercing of the lens. Normally there is no vitamin-A found in the lens of the eye. It’s not supposed to be there, it’s not needed there, and it isn’t there. Clearly then, it is logically impossible for a deficiency in something that is not supposed to be present to cause the disease condition in the lens.
In conclusion, it may be stated that vitamin-A has not been isolated from the lens nor is a deficiency of it known to produce any changes there.
Source: MALNUTRITION and THE EYE, page 36
Obviously, there is absolutely no image processing connection here in the outer tissues with vitamin-A, or vitamin-A deficiency. Yet, when a disease condition shows up in the tear ducts, the conjunctiva, the sclera, the cornea, and even the destructive piercing of the iris and lens, they are almost immediately blamed on (oh, umm, but it depends on what country you live in) vitamin-A deficiency.
McLaren makes a similar observation in his 1963 book.
There is a number of puzzling things about the way in which the eye is involved in vitamin-A deficiency. The main obstacle to an understanding of these matters is undoubtedly our present ignorance of the role the vitamin has outside the retina.
Source: MALNUTRITION and THE EYE, page 75
Therefore, no, sorry, vision is not a chemical process, rather it is an electrical (analog-to-analog) process. The eye is an extremely sophisticated digital reception organ. Retinal in the eye receives incoming light energy, and that light energy induces a potential (a voltage) in the photoreceptors. The voltage and its amplitude and oscillation frequency vary with the light’s intensity and wavelength. The retinal molecule obviously must stay continually intact during this process. Repair and replacement would probably occur only while sleeping. And no, nature is no fool. There is no way nature would build the most precise, and most exquisite organ in the body with a critical dependency on it needing to be continuously refueled by a potentially highly toxic and cancer-causing molecule. There is no chance of it. It’s back to the drawing board on that one guys.
|
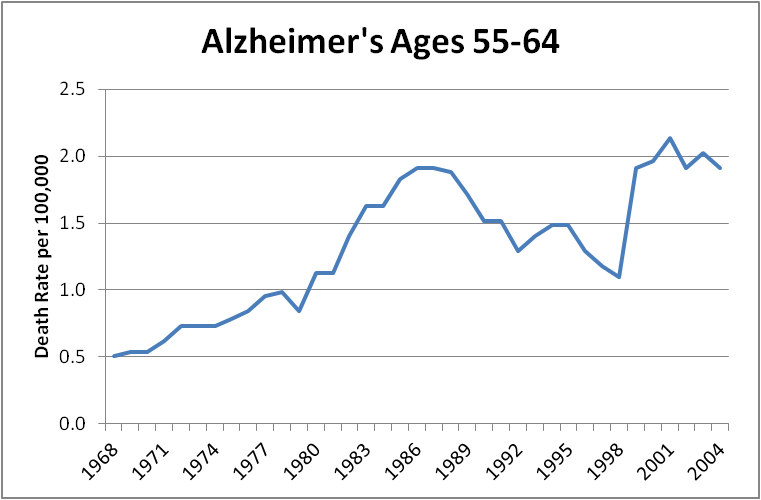
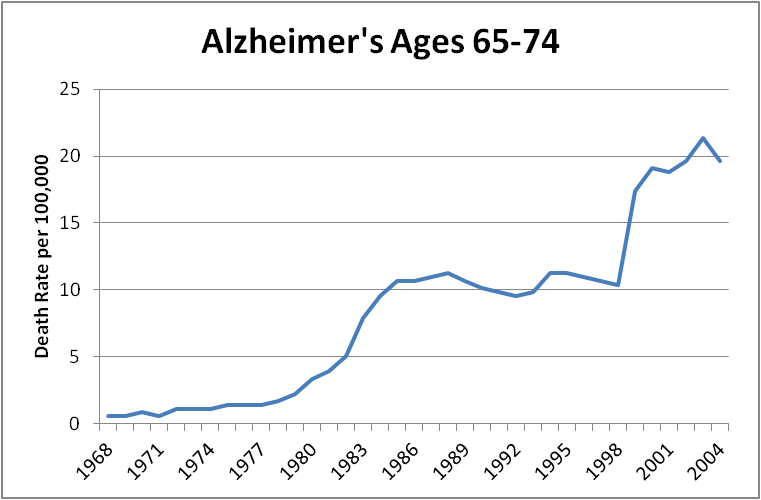
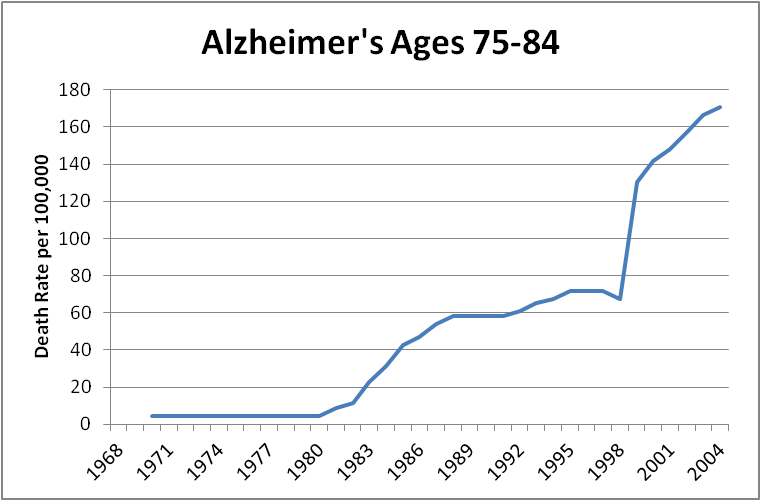
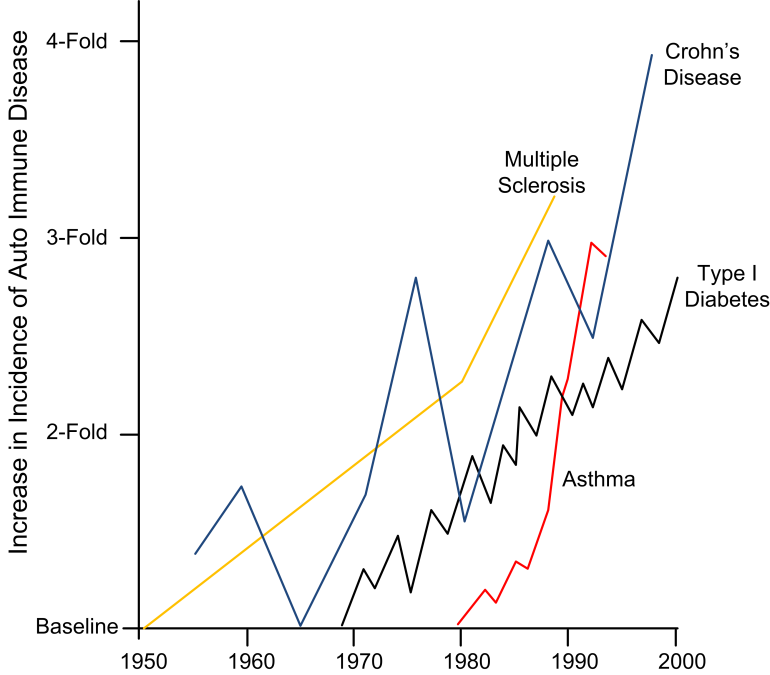
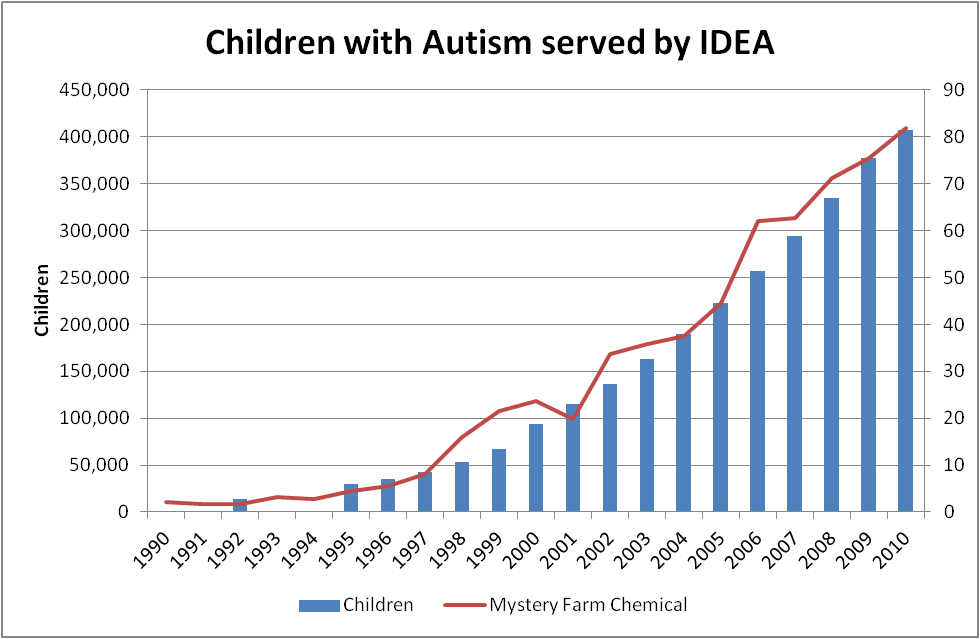
When I started my investigation of potential root causes of eczema and started to piece that together with Crohn’s and Alzheimer’s disease one of the very first things I did was to look for data on incidence rates from around the world. Being from completely outside of the medical sciences field, I only had a vague understanding that the disease rates in North America were somewhat higher than some other regions of the world. I might have guessed that there might be some anomalies in the range of, oh say, 0.02 %. After all, we are the most well-nourished, well medicated, most vaccinated population on the planet. Moreover, we have some of the best sanitation and medical support systems in the world. Generally speaking, I thought that maybe our soft lifestyle, with not enough exercise, could account for a slightly higher disease rate. However, within less than two hours of investigation, I was completely stunned by what I was finding. North America has some chronic disease rates that are 50, 200, and even 400 times higher than many other countries. Our cancer rates are also like 50 and 200 times higher too. Since the 1860s our cancer rates have jumped to being between 500 to 1000 times higher now too. Just to be very clear, that’s not 500 to 1,000% higher. No, it’s a whopping 50,000% to 100,000% higher. In the context of recent history, say over the last 100 years or so, the rates of the “autoimmune” diseases in North America are easily now 500 times higher too.
I was completely blown away, and just shocked by those numbers. Being an engineer, seeing anomalies in the range of say 0.1% are usually notable events. So, therefore for me to now see disease rates that are 20,000% and 40,000% higher in North America was just overwhelmingly stunning. Somehow, the dramatic rate increases for most of these diseases started between the mid 1970s and the early 1980s. Also, clearly keep in mind that these years are not the genesis of the disease. No, these diseases did exist well before these dates. A hundred years ago, these diseases did exist. Except, back then there were only extremely rare incidences of them.
| Table 4 Example disease incidence rate disparities by country | |||||||
|
Disease |
Western Country |
Rate per 100,000 |
Non-Western Country |
Rate per 100,000 |
Ratio |
Source |
|
| Alzheimer's | Finland | 53.77 | Singapore | 0.19 | 283.0 to 1 | 19 | |
| Alzheimer's | USA | 45.58 | Georgia | 0.25 | 182.3 to 1 | " | |
| Crohn's | Denmark | 225 | Puerto Rico | 6 | 37.5 to 1 | 20 | |
| Crohn's | Canada (NS) | 202 | China | 3 | 67.3 to 1 | " | |
| Celiac | Finland | 1900 | Turkey | 900 | 2.1 to 1 | " | |
| Ulcerative Colitis | Denmark | 378 | Lebanon | 6 | 63.0 to 1 | " | |
| Thyroid - Hyper | USA | 500 | Iran | 20 | 25.0 to 1 | " | |
| MS | Canada | 291 | Pakistan | 10 | 27.0 to 1 | " | |
| Sjögren’s | UK | 3500 | China | 330 | 10.6 to 1 | " | |
| Autism | USA (New Jersey) | 1060 | Oman | 14 | 75.7 to 1 | 21 | |
What is the most important thing these charts are telling us? They tell us with crystal clear clarity that these are environmentally induced diseases. These diseases are not rooted in genetics at all. The doubling rates are now faster than the human reproductive cycle. They are not due to aging, or almost not at all. We have simply been confusing aging with exposure time. Even Alzheimer’s is doubling in multiple age groups too. Kids are getting autoimmune diseases at growth rates just as high as any other age groups, if not higher. We also know, with a high degree of certainty that these are not infectious diseases, and they are not cancers. These exponential growth rates are almost unique to the industrialized world and are not repeated in many other regions of the world such as India, China, Pakistan, Russia, etc. Table 4 highlights just some of these numbers.
As if these numbers are not bad enough, we need to factor into them the significant immigration to North America and other Western countries over the last 20 to 30 years too. This fresh influx of healthy people will have reduced our statistical incidence rates. Therefore, the real numbers are not 60, 75, and 283 times higher. They might be more like 80, 90, and 400 times higher than what is obviously normal for the human population. Yet, when people do emigrate from these non-Western countries to North America they slowly begin to get these diseases at the same rates as us. To get a better appreciation for the significance of the situation, let’s look at some of the rate differences graphically.
19 http://www.worldlifeexpectancy.com/cause-of-death/alzheimers-dementia/by-country/
20 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2783422/
21 http://sfari.org/news-and-opinion/news/2011/researchers-track-down-autism-rates-across-the-globe
|
Figure 19 Some chronic disease incidence rate disparities per 100,000 |
||||
|
||||
|
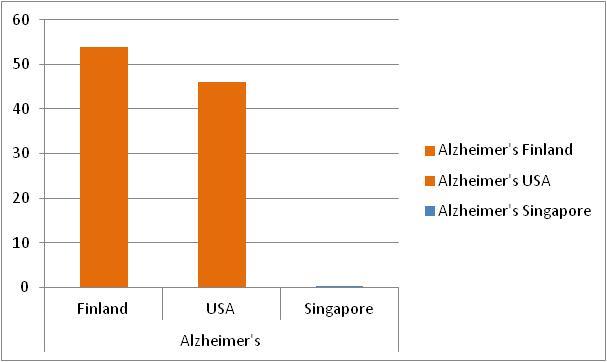
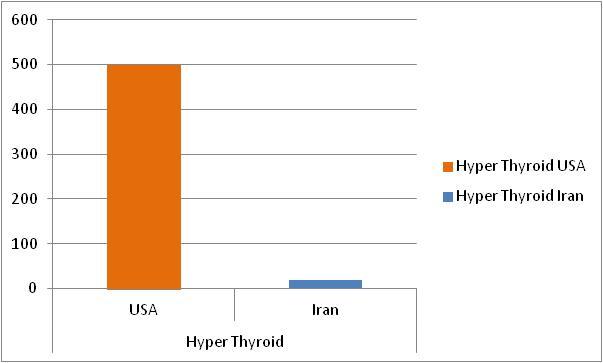
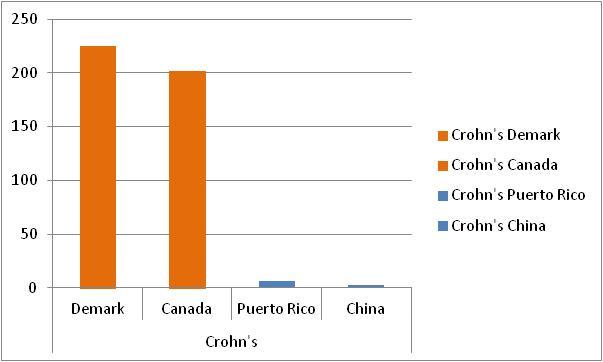
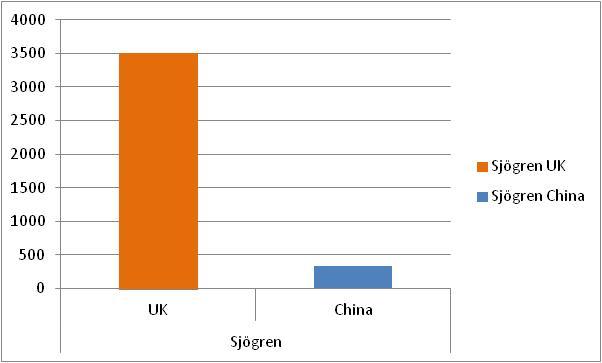
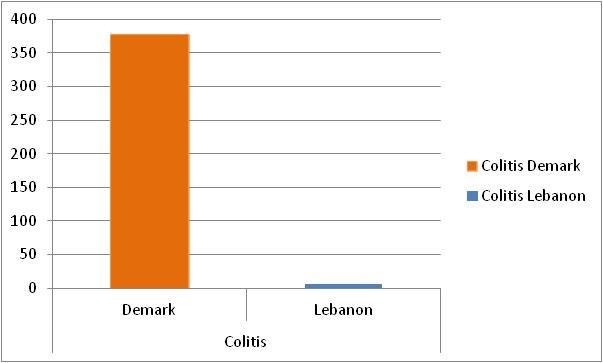
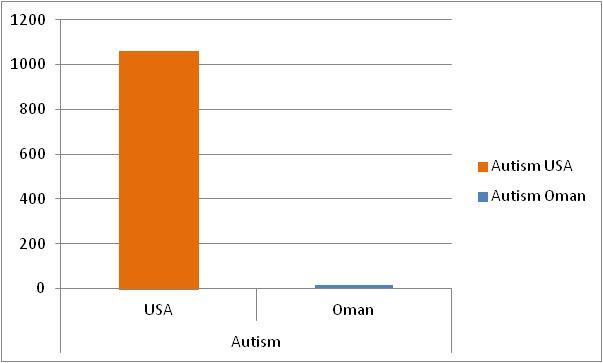
Now, for researchers working in the health sciences, looking at each one of these diseases in isolation, these rate disparities might appear to be rather mysterious. However, when you look at all of this data combined, there’s no mystery at all; these are simply environmentally caused poisonings. There is no way anyone can call that an anomaly. Additionally, many of the disease incidence rates are currently following an exponential growth curve, and that is just downright alarming. What in the hell is going on here? Why is this information not all over our news media?
I have absolutely no doubt that many senior scientists and officials in government are all too aware of the extent and scope of the rising disease epidemics we are facing as nations. But, of course, our governments, and the medical establishments, and therefore our news media don’t want us to know this information. Here in Canada, I quickly found some very strong evidence that indicated not only is the Canadian government not alerting people to these little facts; they are deliberately attempting to cover it up and obfuscating it too. And, of course they are, because if we all became aware of this shocking information, many people with the financial means would flee the country. It would be even more damaging if the true rates of these hidden plagues became general knowledge outside of North America. If that took hold, new immigrants would stop coming here. Having that happen would be an absolute disaster for our economies. Therefore, yes, these astounding disease rate disparities needs to be hushed up.
However, somewhat counterintuitively, there’s an amazing gem of good news hidden here in the bleak stats on the North American disease rates. That amazing gem of good news, if not fantastically good news, is that the chronic disease devil has just revealed his hand. He’s gotten a little too greedy, and we now know his identity.
As far as I can discern, the current, and official explanation behind many of the chronic diseases is the “bad-luck” theory of disease etiology. Basically, what many people in the general public are told is: “Oh, it’s nothing you’ve done wrong, the reason you have this disease is just bad-luck.” Naturally, that explanation is rather pathetically weak. So, for those in the medical, and scientific fields, the excuse is somewhat expanded to it being due to some vague combination of lifestyle, genetics and some environmental factors as being the root cause. Once again, there’s no doubt that government and medical researchers know full well this is just the officially supported propaganda version of the story. Of course, once you see disease rates that are 40,000% higher in North America, that official explanation completely falls apart and is so obviously utter bullshit! It’s a big fat lie used to cover up the colossal failing of government and the medical establishments in finding the true cause(s). The real truth that they don’t want you to know about is that it is 100% environmental factors that are causing the new disease plagues we are now facing. It is something very tangible here that is causing these insanely high disease rates. Seriously, even a 10-year-old can figure that one out.
But, for me at least, I could have never imagined that we had such glaring rate differences like this. Like so many other people outside of the medical profession, I was almost completely blind to the fact that this was indeed the case. Therefore, when I saw numbers for some of the disease rates being 20,000% and 40,000% higher in North America versus other countries, it was stunningly obvious why this has happened. The rate difference is so outrageously abnormal; it means there is only one possible explanation, and that is that the chronic diseases are chronic poisonings. Additionally, it is critically important to understand that I am not talking about just the differential disease rates as being poisonings. No. I am talking about the root cause of all incidences of the disease as being poisonings. And that is fantastically good news. Like I said before, the devil has now revealed his hand.
Just to make the point clear, let me use diabetes as an example. Let’s say the diabetes rate in China is 2 in 100 people, and in North America, the diabetes rate is 50 in 100 people. I am not saying that the extra 48 in 100 people getting diabetes in North America are having their diabetes being caused by some environmental poison found in North America. No, what I am saying is that all cases, all the 50 in 100 people in the North America group, and all 2 in 100 people in the China group, are having their diabetes caused by a poisoning. In other words, diabetes is a poisoning. Eczema is a poisoning. Crohn’s disease is a poisoning. Arthritis is a poisoning, and so is Alzheimer’s and so are almost all the other autoimmune diseases. This statement is not some trivial, or trite remark. It is not grasping at straws or wishful thinking. Rather it is simply a fact. Something here, in our environment, is poisoning us into the diseases.
If it helps, just think of the worldwide human population being a large lab experiment. In the experiment, and in just one region of the lab, the disease rates are 20,000% and 40,000% higher. Clearly then, that’s not bad-luck, that’s not poor lifestyle choices, that’s not genetics. No, it’s poisonings; there is simply no other plausible explanation. Period, end of debate.
Moreover, even after spending just a little bit of time thinking about the so-called autoimmune diseases (regardless of the regional differences in incidence rates), it is just stunningly clear that they are poisonings. That’s because the human body simply will not just magically, and spontaneously, self-destruct like this. It is biologically impossible for us to be here on the planet as a species if we had this inherent flaw and tended to spontaneous self-destruction rather than to self-repair and trend toward health. As a biological being, the goal of the organism is to survive as long as possible, and to remain as healthy as possible, and to be as reproductive as possible. We are (were) perfectly well adapted to our environment. Therefore, the great epiphany for me was that there is only one way for us to move into (non-infectious) chronic disease and that is for us to be chronically poisoned. That is simply as close to being a biological fact as you can get.
I wish I could claim that I was the first to come to this understanding, but of course, I am not. There are many other people who have come to the same realization. But, one guy stands above the crowd on this matter. He not only established this concept, he even taught it in medicine over 2,500 years ago. Yes, this is none other than Hippocrates.
Illnesses do not come upon us out of the blue. They are developed from small daily sins against Nature. When enough sins have accumulated, illnesses will suddenly appear.
Hippocrates
Today, Hippocrates is regarded as the father of “modern” Western medicine. But modern Western medicine today only pays lip service to the teachings of Hippocrates. For the most part, Western medicine doesn’t actually believe, or practice, any of his teachings. The truth is that modern Western medicine is now so completely perverted it is in total violation of Hippocrates’ teachings. So much so, that if Hippocrates were alive today, and seeing that the absolute standard practice in “modern” medicine attempts to poison people back into health, it would make him sick with repulsion.
What I want to be very clear about here is this reference to Hippocrates’s understanding of disease is not just some clichéd notion, and I am not trying to impress you with celebrity name-dropping. Rather, it’s to get you to both appreciate just how brilliantly correct Hippocrates’ was, and how critically important this fundamental understanding is.
We can draw an analogy here to that of Newton’s first Law of Motion. Newton’s law states:
|
“Every object will remain at rest or in uniform |
Hippocrates's version of the similar law of biology is that:
|
“A person is going to remain in good health |
Hippocrates's brilliance in this regard is close to being on par with Isaac Newton’s. But, for him to then determine that once a person has become sick with chronic disease, and to continue to feed themselves is to feed their disease is pure genius. He clearly understood that chronic disease was a chronic poisoning sourced from foods. Of course, both Newton and Hippocrates were brilliant geniuses, and they both uncovered these laws of nature through keen observation, and by simply thinking about it. Chronic disease in the human body is not normal. If we have chronic disease, then we have chronic poisonings. That is the greatest understanding in medicine, ever.
Of course, now that chronic disease is so incredibly common, we’ve been acclimatized and deceived into believing it’s normal. What so-called modern medicine has failed to see, in the face of more than 70 years of overwhelming and escalating evidence, and what was taught 2,500 years ago, is that our chronic diseases are indeed chronic poisonings.
That failed understanding, combined with greed and corruption, has steered medical science into attempting to treat the chronic diseases, and therefore chronic poisonings, with “drugs.” Of course, with regards to the chronic diseases the “drugs” have never worked very well, and at best only delay or mask the symptoms. Naturally, the drugs can’t work, because we don’t have drug deficiencies, we have poisonings. But, don’t take it from me that the drugs are not working, here’s a quote from a recent book from a top pharmaceutical industry researcher and academic. He’s also extremely supportive of the pharmaceutical industry.
Vast hordes of researchers are working to find cures for nearly every disease known to medicine. With these keen intellects working diligently, competing fiercely to solve these mysteries, you would expect that no stone has gone unturned, no avenue unexplored. Yet, we have not found cures for most types of cancer. Other diseases, including Alzheimer’s, Huntington’s, Lou Gehrig’s, and Parkinson’s, remain depressingly void of curative therapies. Why?
Brent R. Stockwell; Columbia University Press, Jan 15, 2013 – Science; Page 4
Of course, the same dearth of cures applies to all the autoimmune diseases, diabetes, arthritis, obesity, autism and many more diseases. But, it’s not for lack of drugs, because there is now a ridiculous number of FDA-approved drugs on the market, and somewhere in the range of 20,000 drug products that are currently on the market. Yet, in his book, Brent Stockwell says we are in crisis - because we don’t have enough new drugs in the development pipeline. To summarize it, his view is that our health crisis is because we don’t have enough drugs. He goes on to explain the industry has drugged every cell in every imaginable way, and almost nothing is working. Therefore, the next Holy Grail in medicine is to drug the undruggable - the cell proteins – and drug all 20,000 of them too. That’s right; he thinks we need to discover another 20,000 drugs, and drug every cell protein in every imaginable way. In my humble view, that is complete and utter insanity.
Not to be dissuaded by the little fact that their drugs are not actually working, Stockwell gushes about the big “blockbuster” success stories in the industry. Naturally, his use of the term “blockbuster” applies only to the drug’s sale and profit numbers. The great showcase drug category he uses to expound on this point is the Benzodiazepines. It’s been a great molecular success story for the industry because they can just stack up another benzene ring on to the base “scaffolding” and from there get additional drug patents. With that, the marketing and sales teams sell the hell out of it, and the companies make great fortunes. Of course, what Stockwell doesn’t mention is the staggering number of deaths the wonderful “Benzos” are causing each year. He does not tell us that their fantastic “Benzos” are now killing about 7,000 American’s each year. The shocking reality is that the annual kill rate from the Benzo based “medicines” is higher than the combat death rate that American soldiers faced during the Vietnam war! So, this “blockbuster” supposed success story is simply more killing for profits.
Moreover, if you read Stockwell’s book you’ll discover that the science used in their great “Quest for the Cure” is about on par with using an Ouija board or medieval witchcraft. And sadly, that’s not hyperbole. Just to add insult to injury, the drugs themselves are more often than not actually additional poisonings too. Because many of the drugs are indeed poisonings, that is why they almost always have so-called “side-effects.” Therefore, and very ironically, if not bizarrely, modern medicine is attempting to treat chronic poisonings, with more poisons. So, is it any wonder that most people just remain sick and diseased, and many slowly die anyway? We simply don’t need drugs to cure the human body; we just need to stop poisoning it.
The natural healing force within each one of us is the greatest force in getting well. Our food should be our medicine. Our medicine should be our food. But to eat when you are sick is to feed your sickness.
Hippocrates
Therefore, (non-infectious) chronic disease is never normal. It is manmade, every single time. It is being caused to happen. The current “bad luck” theory of disease etiology propagated by the medical establishment is complete rubbish. They are deliberately hiding the truth. The truth is that our foods are indeed somehow causing our current disease rates. Period. But, if you have any doubts about this conclusion, don’t bother asking most physicians, or so-called researchers that are part of the medical establishment. Rather, go ask mathematicians, engineers, or others in the physical sciences to analyze just the incidence pattern data. The incidence pattern is in no way random. Therefore, the cause of these diseases is not random “bad luck.” It will be clear to them that the diseases are being caused by our environment.
However, you don’t even need to be a scientist to see what’s truly going on here. You can present these facts to anyone with a bit of common sense and the ability to think logically, and I think they will see it. When you give them the raw data, and the very basic facts about our astonishing disease rate disparities, I believe they will come to see the truth in it. Our chronic diseases are indeed poisonings.
Of course, the cynics and nay-sayers will still throw up all kinds of distracting excuses to claim otherwise. One of the excuses always cited is claiming that our disease epidemics is caused by our “bad” lifestyle choices. They’ll claim that it’s our bad diets or lack of exercise, etc. that is causing the disease rate increases.
But, you can rule out this claim in two minutes of investigation, and by applying a trivial amount of logical thinking. You can immediately rule out this excuse because small children are now at the battle front in this disaster. They are taking the brunt of the onslaught of the rate increases in these very same chronic diseases. Our nation’s young children are now getting autoimmune diseases at record rates. Infants and one and two-year-old kids are getting diabetes, Crohn’s, colitis, asthma, eczema, chronic infections, leukemia and other cancers, obesity, and even eye diseases at astonishing rates. This rate, and the rate increases, of disease is biologically impossible to be a random event occurring in just North America.
These children are well cared for, well-nourished, and loved. They are not getting these diseases because of neglect, or sneaking off and eating too many meals at say McDonald's, or not getting enough exercise. In Canada, we now have two-year-old kids getting Multiple Sclerosis; we’ve never seen this happen before. MS used to mostly only strike women in Canada when they were in their 50s or later. Therefore, it should be 100% clear to anyone, and everyone, that these diseases are poisonings. Kids are being hit with the worst of it because they are smaller, and are just more susceptible. It should be almost biologically impossible for our kids to be getting these diseases at all. The only plausible explanation is that external influences are causing the disease. When external influences cause disease, it is called a poisoning.
Likewise, it’s nearly biologically impossible for an even remotely adequately nourished human baby to just suddenly and spontaneously die (SIDS). There is absolutely no way that this can normally happen in the species at the very pinnacle of biological evolution on the planet. Humans are not this weak and frail. Kids do not die from “nothing.” No way, not a chance of it. So, for the pediatricians out there who can’t figure this out, simply put, SIDS is kids that have been poisoned to death. Like the autoimmune diseases, SIDS is a phenomenon almost unique to the developed countries of the Western world too. Shockingly, it is now reported that the USA has the highest first-day infant mortality rates of the industrialized world.22
Naturally, once kids start showing the signs and symptoms of this sinister poisoning, what do the esteemed medical professionals do? They most certainly don’t get to the root cause of it; no, of course not; they simply dose them up on more toxic drugs (a.k.a. poisons).
An analysis of 2013 IMS Data, found that over 274,000 infants (0-1 year olds) and some 370,000 toddlers (1-3 years age) in the U.S. were on antianxiety (e.g. Xanax) and antidepressant (e.g. Prozac) drugs. This report also found over 1,400 infants were on ADHD drugs.
Source: http://blogs.wsj.com/experts/2015/02/19/why-are-so-many-toddlers-taking-psychiatric-drugs/
Thus, we, as a nation, are simply poisoning our kids into disease and early death. Once again, there’s no drama intended with that statement; it’s just a fact.
Now, let’s apply Hippocrates’ ancient knowledge to today’s modern chronic diseases and determine which of them are indeed chronic poisonings. To do so, let’s define some basic criteria for this determination pertaining to a named disease.
- It is known to be not caused by an infection
- It has significant variations in worldwide incidence rates. Or, in other words, it presents in significant geographic or even regional clusters.
- It has made a dramatic increase in incidence rates over the last few decades.
- It has moved significantly lower in the average age of onset over the last few decades.
- Small children, and / or teenagers are now getting the disease at rates never seen before in their age groups.
Here are just some of the diseases that match these criteria, and that I therefore have no doubt about them being poisonings.
|
|
Here are a few other diseases that don’t quite match the above listed criteria, but I also have absolutely no doubt about them being poisonings too.
- Breast Cancer
- Parkinson’s
- Cataracts
- Heart disease & Stroke
- Osteoporosis
- Hip joint failures
- SIDS
In one of my early blog posts I commented that now after being vitamin-A free for an extended period of time and that nearly all my health conditions had resolved, the most logical test of my theory would be for me to directly reintroduce vitamin-A back into my diet. To try to isolate it down to this one factor the reintroduction of vitamin-A would need to come directly from vitamin-A pills and not from a food source. Of course, I had no great desire to do that. No, not even in the name of science. In my blog post, I stated that I was too chicken-shit to do it. Naturally, there’s a very thin line between bravery and foolishness. Moreover, at my age, I really did not feel like risking reintroducing all those disease conditions. Therefore, I was hoping a younger person would take up this challenge. That did not happen.
Next, I think I got a little too complacent. Maybe, now living in very nice smooth skin, having near perfect 20/20 vision, good stamina, no fatigue, no joint pain, and enjoying good health, and most importantly no eczema, I had forgotten about just how bad things were. Additionally, by this time much of my gray hair disappeared and had gone back to my natural black color. So, with all this good fortune maybe I was feeling brave enough to add some vitamin-A back into my diet? Nope, I just foolishly believed and was misinformed by another bogus bit of medical science.
Around that point in time, to investigate the early history of vitamin-A and its relationship with vision I was reading numerous medical textbooks on the topic. I came across information on lutein/zeaxanthin and how it was another supposedly essential nutrient required for eye health. Lutein and zeaxanthin are carotenoids and are not considered to have vitamin A activity because they are not converted to retinol. Additionally, lutein and zeaxanthin are the only carotenoids that concentrate abundantly in the eye, and are thus thought to have a protective function. Lutein and zeaxanthin particularly collect in the inner layer of the retina, the macula, and appear to be found in a lower concentration in the retina of people with age-related macular degeneration.
Clearly, being on my very restrictive diet, I probably wasn’t getting any of these two carotenoids. Therefore, on one of my shopping trips to pick up some vitamin C, I saw lutein/zeaxanthin on the vitamin shelf and decided to add it to my diet. Well boom, wouldn’t you know it. It hit me like a speeding truck. Actually, it was more like a speeding truck that was on fire. Within a week, I had severe arthritis developing in my left hand. In a few more weeks, things were going seriously wrong. So much so, that the knuckles on my left hand started to literally grow out of the palm of my hand. The bones in my left wrist became swollen to about twice their normal size. The skin on the backs of my hands quickly became significantly inflamed again. My eyes became swollen and developed a severe amount of vascularization. My hair quickly went from being about 90% black to once again being about 70% gray. I developed an intense amount of inflammation in my pelvic area. The skin on the sides of my torso was becoming bumpy, almost rash-like. I had a massive, and almost unbelievable, amount of skin shedding off the backs of my hands.
I initially thought that my overall experiment was making a big reversal and was now failing. Of course, I kept on reminding myself that if an experiment fails to prove a theory, then the theory is wrong. But, then I went back, and did a little bit more reading about this wonderful lutein. And wouldn’t you know it, lo and behold, it’s categorized as another form of vitamin-A. I thought “great; I just dosed myself up on the very thing that I thought I would never do”; more vitamin-A. This mistake wasn’t quite foolishness, nor bravery, on my part. It was just my response to more disinformation and more bad science. I stopped taking the lutein, and within four days my inflammation condition started to calm down, and I started to very slowly return to normal.
However, for me, the damage was done. My knuckles and skin had been seriously damaged again, so had my eyes. It’s taken me at least five months to fully recover from that little indiscretion. Quite amazingly, my hair is now once again returning to being black. Therefore, although lutein is commonly recommended to senior citizens for macular degeneration, I consider it to be nothing more than another poison, and a death trap for seniors. But, let’s not blame individual physicians for making this unfounded recommendation because its comes straight from the de-facto authority, the National Institute of Health.
Age-Related Macular Degeneration
Age-related macular degeneration (AMD) is a major cause of significant vision loss in older people. AMD’s etiology is usually unknown, but the cumulative effect of oxidative stress is postulated to play a role. If so, supplements containing carotenoids with antioxidant functions, such as beta-carotene, lutein, and zeaxanthin, might be useful for preventing or treating this condition. Lutein and zeaxanthin, in particular, accumulate in the retina, the tissue in the eye that is damaged by AMD.
Source: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/
That’s correct, without knowing AMD’s etiology they make this completely unsupported extrapolation that just having the accumulation of lutein, and zeaxanthin showing up in the retina that it might somehow be beneficial. Bizarrely, what they don’t appear to ask is if the accumulation of lutein and zeaxanthin in the retina might not actually be causing AMD.
And, oh yes, from my firsthand experience with it, it probably is. It’s also caused a whole lot more tissue damage outside of the eye too. So, to any medical professionals out there who might happen to read this, please stick this bit of new science directly in your eye and stop prescribing lutein/zeaxanthin. Yes, this is also reasonably conclusive evidence that vitamin-A caused all my original horrible disease conditions. That includes eczema, arthritis, brain fog, cataracts, osteoporosis, kidney disease, diabetes and more. And if you happen to think that this one little case study doesn’t prove anything then you are wrong. This condition is a medically documented state that men of my age can get into. It is documented as getting into a state of such saturation with vitamin-A that the body cannot tolerate even small amounts of it.
Some individuals seem to suffer from vitamin-A intolerance, that is, the appearance of signs of toxicity upon routinely ingesting moderate amounts of vitamin-A. This relatively rare condition, which seems to be genetic, mainly affects males.
Source: Vitamin-A Deficiency; Health, Survival, and Vision; See: page 244
With that information, and it has been known since at least 1996, why the hell isn’t the medical community warning senior citizens about the extreme danger of consuming too much vitamin-A? I guess it would just be bad for business.
What about Sommer’s claim that the condition “seems to be genetic?” Does he have any evidence what-so-ever to support that claim? Has he found the gene for that one? No, of course not. Even though this may appear to be a small point, its significance is crucially important to appreciate. It is a pattern that I’ve repeatedly seen in so much of the so-called medical research. So often when medical science can’t explain something they just simply fabricate these completely nonsensical rationalizations. This tendency to blame disease on genetics is not only an idiotic cop-out that prevents them from finding the real cause. This practice is incredibly, and recklessly, dangerous. No, this is not a genetic condition or disorder. My genetics did not magically change at age 54. Additionally, this is not some mystical “intolerance” either. What’s really happened here is perfectly clear. It is that, for people like myself in this condition, we have simply reached a saturation point of safe vitamin A storage. After that, every little bit of it is a poisoning. Although lutein/zeaxanthin is documented to not convert into retinol and therefore not have direct vitamin A activity, it sure did for me. Or, maybe it just forced other stored vitamin A to be released? Either way, clearly the science behind lutein/zeaxanthin is far from complete.
In my previous e-book, I made the claim that autism is being caused by the subclinical poisoning of vitamin-A. The claim was based on a lot of circumstantial evidence implicating it in the disease. The strongest bit of evidence I came across was the extraordinary rate a spontaneous bone fractures in autistic children. This fact clearly indicated that these kids are under sustained and massive amounts of inflammation. And with there being only one chemical substance known to medical science that can possibly cause spontaneous bone fractures, I felt that I was making a pretty strong connection. However, I was completely living in my own little scientific bubble too. I had no medical knowledge. I had no firsthand experience with autism, knew no one with it, and I knew no family with children with the condition. I was completely new to the topic, and a complete outsider. Yet, here I was making an apparently ridiculous claim as to its cause. However, I believe in numbers, and the numbers told the story. Therefore, this was not at all just a weak opinion on my part. Additionally, I had some firsthand experience with something seemingly unrelated; eczema. It was my experience with eczema, and reading about the high prevalence of eczema occurring with autism that got me started down this path of investigation. From there, I dug just a little bit deeper, and did something that a lot of doctors probably dismiss as being unimportant. I started reading some of the detailed accounts from parents as they witnessed their kids sinking off into this horrible autism condition. Two common observations particularly caught my attention. Firstly, many parents spoke about the “light in their kid’s eye being lost.” Many people might take that comment as a metaphor, but I interpreted it as being very literal. The light in the eyes being lost was directly due to the drying of the eyes, and the loss of the lubricating tear film. The loss of moisture on the surface of the eye prevents light from being reflected from it. Of course, we now know how and why that happens. Naturally, as the surface of the eyes dries it will force the kids to start blinking more often. They are simply attempting to re-lubricate the eye surface. This repeated blinking pattern is the “eye clicking” that many parents report in their kids.
The second very important comment was that made directly from the kids themselves, to their mothers, just before they fell off into a seizure or had their eyes roll up into the backs of their heads. The comment was that they could taste metal in their mouths. And yes, I knew about that happening too, and have tasted metal myself too. I also now know exactly why that happens. It is the iron being drawn out of the blood and liver, interacting with the calcium being used to buffer an acid. Then, there was this list of observations of the Hikan condition Dr. S. Mori of Japan published in his 1904 paper.
- more common in boys than girls
- the younger the child, the more susceptible they are
- diarrhea
- abdominal expansion
- excessive appetite
- night blindness
- xerosis of the conjunctiva (dry eyes)
- thinning of the hair
- dry skin
- sensitivity to sunlight
And, yes, those are indeed many of the same comorbidity conditions reported with autism. Then when seeing that the documented side-effects of high dose vitamin-A supplementation in pregnant mothers was indeed subsequently leading to damaged central nervous systems (CNS) in their children, and especially affecting speech, language, and IQ, it was becoming rather obvious.
Participants also agreed that, after the first trimester, exposure to levels in excess of 10 000 IU of preformed vitamin-A or retinoic acid is less risky. However, caution is advisable because some preliminary data in humans suggest mild abnormalities in CNS related performance (e.g. speech and language, and verbal IQ tests) from exposure to 13-cis retinoic acid during the fetal period of development. These observations, which need verifying, would extend the period for possible toxic exposures into the second trimester of pregnancy.
Source: WHO/NUT/98.4 Safe vitamin-A dosage during pregnancy and lactation, page 20
But, why would anyone think that this exposure risk stops at birth? What about the post birth risk due to subsequent exposure to retinoic acid? What’s going to elevate the retinoic acid levels? High levels of tissue stored retinol, and sustained inflammation will. How about a little nudge from multiple vaccines? And yes, here once again the experts think that abnormalities in CNS related performance (e.g. speech and language, and verbal IQ tests), permanently affecting a child’s brain are just “mild” adverse conditions.
So, I was seeing the pattern, and with those connections forming, I started to investigate the autism topic a bit more. Like with my other research into the chronic diseases, I was surprised by what I was finding. I quickly learned that the field of autism research was even more completely screwed up than that of the so-called autoimmune diseases. There are bizarre and completely ridiculous rationalizations being foisted on the public to explain away the alarming epidemic rates of this disease. One of the most prominent explanations is that it is just due to a broader definition of the spectrum and we just didn’t notice it before. That’s right, the bullshit goes something like this: in the 1960s and ’70s the autism rates were almost the same as they are now, parents back then were just so daft that they didn’t notice their children being completely incapacitated by it. They just didn’t notice their teenagers curled up and confined to their beds, wearing diapers, and sucking their thumbs. Somehow, we just simply missed it. Oh, and then of course, we need to ask what’s happened to all the autistic kids from the 1960s, ’70s and ’80s, once they grew into adulthood. Where are they today? Did all those autism victims just magically disappear?
Therefore, this claim that the rates are about the same as before is such a complete load of crap. It’s ridiculous, and any medical doctor that repeats that nonsense should not only have their medical license immediately revoked, they should have their driver’s license revoked at the same time too. I mean seriously, to anyone with even just two functional brain cells, it is a completely ludicrous suggestion to think that the epidemic rate of autism is not a new phenomenon. Therefore, the exponential rate of autism we are witnessing is indeed very real and it is being caused by something in our environment.
But, there are many other competing theories regarding the autism epidemic. Here’s one that caught my attention.
From 1987 to 1998, the California State Department of Developmental Services reported a 273 percent increase in autistic disorders, while the state population grew only 19 percent. The increase did include cases of high-functioning autism or Asperger's. Many researchers today believe that this meteoric increase is that people who have mild tendencies like engineer’s syndrome are more likely to marry each other. A generation ago, men with engineer’s syndrome would seek out a spouse with superior social skills because they knew they had deficits, but now they are marrying women with the same disposition.
http://www.continuingedcourses.net/active/courses/course067.php
How are these people not profoundly embarrassed and ashamed of publishing such idiotic statements? If that’s any indication as to the depth of thinking and scientific investigation into the etiology of this new epidemic, we are in very, very big trouble. Why is it not just blindingly obvious to the medical establishment that autism simply must be a poisoning?
My personal ignorance of the situation with the autism rates in our society was echoed by my ignorance of the ongoing raging debate regarding the possible implications that vaccines were contributing to, or even causing, this epidemic. I had almost no idea this debate was going on. About a decade prior, I saw a news report about a British doctor, named Andrew Wakefield, who had made the claim of a possible association between autism and the MMR vaccine. However, his claim was quickly “debunked” by the medical establishment, and the doctor was revealed for having committed scientific fraud in the case. Having almost no interest in this topic at the time, I paid little attention to the story. However, I do remember thinking about how odd that story was. I wondered why would the doctor commit scientific fraud in such an important area affecting the health of children? I felt if that proved to be true, it was just so beyond being egregious. I remember asking myself, what could have that doctor’s motivations have been in doing so? It just didn’t make sense to me. Well, it’s a big complicated world, and at that time it did not affect me, and therefore I wasn’t going to worry about it too much. Now, here I am doing my armchair investigation of autism and the autoimmune diseases and the conflation between them and what I am claiming is ongoing medical scientific fraud. As I started this investigation, I was very surprised to find out about how intensely polarized the debate was between two factions. In one camp, the pro-vaccine camp, you have the medical establishment, governments, all the government medical regulatory agencies, nearly every medical doctor, pediatrician, and the clear majority of parents.
In the other camp, you have the “anti-vaxxers”, a much smaller, relatively speaking, a tiny, group of parents who claim their child has been harmed, and/or who have in some unexplainable way “gotten” autism, or other chronic disease, from their vaccinations. Naturally, since this matter affects children’s long term health, this is a tremendously heated debate, with a ton of emotional weight thrown in from both sides.
The pro-vaccine camp claims to have “science” on their side, and that the record stands for itself. It is simply that vaccines are safe and effective, and have saved countless millions. It’s their mantra: “vaccines are safe and effective”, and that “the science is settled”, period. They want us to believe that’s the end of the story, and there’s nothing more to discuss. The pro-vaccine camp claims that the anti-vaxxers are a threat to the national health, and if their misinformed message gets any traction it could cause a resurgence in the epidemics of the infectious diseases that have been nearly conquered. The pro-vaccine camp claims that we all need to be very highly vaccinated to maintain our “herd immunity.”
In the anti-vaccine camp, you have mostly parents with injured children, many of who now have lifelong disabilities, and often autism. The reason the parents in this group believe that there is a causal connection between vaccines and their kid’s health condition, is because they have directly eye-witnessed it happen. Therefore, that’s a very compelling bit of evidence. These parents are rational, loving, well caring parents. Additionally, most were in the pro-vaccine camp before their child’s encounter with the adverse reactions. They had dutifully, and with the best parental intentions, taken what was their perfectly normal healthy child in for routine vaccinations. Where upon, thereafter, their child had quickly cascaded into the disease condition.
If this only happened once or twice, we could dismiss it as being an abnormality, or some weird glitch with the vaccine-kid combination. But, it’s not just once or twice. It has now happened in the tens of thousands of cases. Thousands, and thousands of parents have been recounting the same sequence of events. Thousands of almost identical accounts are being repeated over and over, and from around the world too. Of course, government and industry try their best to hush this up, minimize the significance of it, and have been quietly paying out some monetary compensation to the parents that have the clearest cut cases. What’s a clear-cut case? Well, the clearest cut cases are the ones when the kids drop dead right in the pediatrician’s office within minutes of being given the vaccine. Anything less clear-cut than that, then it’s still debatable.
Secondly, many parents comment that when they call their pediatrician to report their kid is having an adverse reaction, and seizures, in response to vaccinations given just hours earlier, they are told that it’s “normal.” You can hear and read about this over and over by different parents in their testimonials. That’s correct, almost unbelievably, many North American pediatricians now think that it is “normal” for young kids to be having seizures. And, of course, it is deemed to be just a coincidence that the onset happens shortly after a round of vaccinations. So, when did it become “normal” for so many kids to be having seizures? Of course, it is not “normal” at all.
In the face of that overwhelming evidence that there’s clearly something drastically wrong here, the pro-vaccine camp steadfastly sticks to the claim that vaccines are safe and effective. The fear of a potentially wide spread infectious disease is so great, there can be no questioning of vaccine safety. Therefore, a very big factor in their science claim is based on fear.
So, even though they claim to have “science” on their side, they are doing something incredibly unscientific. They are taking the ostrich approach to the problem, and sticking their collective heads deep into the sands of denial. They are simply trying to close their eyes to the new mountain of real-world evidence rising up in front of them. But, the pro-vaccine camp does have a large amount of evidence in their favor too. That is, there are millions of kids who get vaccinated every year, and the clear majority of them appear to sail through it completely unharmed, and of course protected from the vaccines targeted infectious microbe (well, at least we are told so).
The other bit of evidence the pro-vaccine camp has on its side is the claim that there’s no scientifically plausible biological explanation for how a small vaccine jab could cause such a devastating prolonged disease, say such as autism. That, on the surface of it, just does not appear to be logically possible.
Now, to me, this sounds all too familiar. I think even a 9th grader can see the obvious irony, and fallacy in that claim of there being no scientifically plausible biological explanation. The material fact is that the small vaccine jab does indeed sometimes cause a devastating prolonged disease condition, and many times even death. That is simply an absolutely and undeniable fact because it is happening. Obviously, there is something going on with vaccines that we simply don’t yet understand. Their claim of there being no plausible scientific biological explanation connecting vaccines and autism implying that there isn’t one is so utterly absurd. It would be equivalent to engineers and physicists claiming that gravity doesn’t exist because we have such a hard time explaining how a force can be applied across empty space. Of course, gravity does exist because we see it in action every day and it keeps us on the planet.23 Likewise, of course, vaccines are causing autism because it’s been eye-witnessed to happen tens of thousands of times over, and it’s being re-witnessed to be doing so almost every single day. Additionally, many parents have before and after videos showing their child’s descent into this hell post vaccination too. Therefore, to deny that vaccines are causing it to happen is simply being astoundingly idiotic.
So, if the pro-vaccine camp claims to have “science” on their side, then great, let’s deal with real science and real facts. Denials, rhetoric, and ad hominem attacks are the domain of ignorance, and have no place in real science.
23 And, yes, thanks to quantum physics are can we can now explain how gravitation forces act across empty space.
Science is the search for, and hopefully the discovery, and the subsequent understanding of the laws of nature. Very sadly, the folks in the pro-vaccine camp are most certainly not on the search for the discovery and understanding of how vaccines are causing autism and the autoimmune diseases. Therefore, the pro-vaccine camp’s claim of having “science” on their side is simply a falsehood and propaganda. Furthermore, since science is not an elitist club, a religion, or a secretive cult, they do not magically have a default monopoly on science either.
The ultimate authority on science is nature itself and nature is clearly showing us that they have not discovered the laws and forces of nature involved here. The fact is that vaccines do sometimes cause a devastating prolonged disease condition. Vaccines do sometimes cause autism. Vaccines do maim and kill some children. Nature is demonstrating that it can and does happen, and it happens rather often too. Thus, vaccines causing autism is therefore an absolute scientific fact because nature is demonstrating it to happen. No amount of denials, rhetoric, and hand waving by the so-called experts can change that fact. Sequestering off this information from the general-public will not change the facts either.
Just because they don’t understand the process, does not mean that it does not exist. Therefore, the claim of there being “no plausible biological explanation” does not mean there isn’t one; it just means it has yet to be discovered. And, of course there is a biological explanation, we just need to find it. There can be zero doubt that it is there, and it will be found. It is just a matter of time. That is a basic logical fact.
Fortunately, you don’t have to wait too long for it either because the real causal mechanism and process is going to be documented over the next few pages. Also, please remember from our golden rules for conducting experiments, if an experiment fails to prove a theory, even once, then the theory is wrong. Our national widespread vaccination programs of our children are indeed a grand experiment, and it has catastrophically failed tens of thousands of times. That is another scientific fact. Therefore, the theory that vaccines are safe, is simply dead wrong. A much more accurate claim would be that vaccines are somewhat safe, but not all the time. The other theory that vaccines are effective, has also been proven to be wrong.
So now, given this information, what would responsible government regulatory agencies do to investigate these anomalies? I think the most obvious thing to do would be to study a large sample of children who have had no adverse reactions to them. Then comparatively, and very carefully, look at the group of children who have being given the same vaccinations and have indeed had an adverse reaction to them. To be clear, this is not studying the vaccinated versus unvaccinated children. No, what we want to find out is why do only some children have an adverse reaction. Therefore, we want to most particularly, and most thoroughly, study the ones who have had the adverse reaction. What’s even slightly, or subtly, different about these children? What’s this so-called “adverse reaction” really and what’s its mechanism? What’s the fundamental underlying condition that causes them to have such drastically different outcomes? Surely, any legitimate scientist should be incredibly curious as to why that is? Who knows where this investigation might lead to? If they went looking for it, they’d surely find the answers.
Of course, to the government agencies, the medical establishments, the vaccine manufactures, and the pro-vaccine groups, that’s the very last thing they want anyone to do. They need to stay on message, and never show any doubts. So, they really don’t want to even begin to think about considering such a study. Because, just beginning it will force them to admit that there’s a known problem. No, they’d rather be seen to be right, than to get it right. But, since nature, the ultimate authority on science, is repeatedly demonstrating that vaccines do harm kids, cause autism, and sometimes even death, their claim to having “science” on their side is simply a blatant lie. Obviously, this position makes them anti-science. Obviously, they’d rather continue to randomly kill and harm children than to get their “science” right. What’s really going on is nothing less than well-orchestrated medical establishment fascism.
So, who’s correct in the grand debate. Well, both camps are somewhat correct, within their own contexts. On one hand, yes, vaccines are probably mostly safe. On the other hand, yes, vaccines do maim, injure and kill thousands of kids each year. But, wait just one minute, doesn’t this sound a bit like what’s going on with the vitamin-A supplementation programs? It sure does to me. It’s the same story:
- “Yes, some kids must die to save the many.”
- “It’s all for the greater good.”
- “A few kids dying is not statistically significant.”
- “Yes, there’s a problem, but we are too busy saving the world to investigate it.”
There are other startling parallels here too. In both cases, the presumed experts are conducting massive health intervention programs that are indeed killing thousands of children year after year. In an astonishing display of scientific arrogance and indifference, they believe only they know best. In both programs, they are so sure, so certain, of their so-called science, there can be no questioning of why the treatments are killing children. Therefore, they are also very willing to make the great sacrifices of randomly killing other people’s children.
But, the parallels don’t stop there. No, the position from the “experts” in these disease conditions is shockingly similar too. The “experts” in the autoimmune diseases publish statements such as: “We, the experts, don’t know what’s causing the autoimmune diseases, and we pretty much don’t even have a clue about it, yet we somehow know that they are not caused by foods.
Since we do not know what causes Crohn’s and colitis, there is no known cure – yet. We do know that your diet did not cause inflammatory bowel disease, nor will a “miracle diet” cure it.
Source: Crohn’s and Colitis Canada
In the context of autism, it’s commonly statements such as: “We, the experts, don’t know what’s causing autism, and we pretty much don’t even have a clue about it, yet we somehow know it is not caused by vaccines.
We don’t know what causes autism. That’s fair to say. We are not sure in the scientific community what causes autism. But, we know that vaccines do not.
https://www.youtube.com/watch?v=_0EMowuPf7I
If these oxymoronic statements aren’t bad enough, it gets shockingly worse. In the case of the autoimmune diseases, hundreds of thousands of people regularly report that certain foods cause them to go into disease flare-ups. This is a fact. It is also completely accepted to be a fact by the medical experts, yet they refuse even to consider that foods are at the root cause. Specifically, regarding the vitamin A supplementation programs, the so-called experts have repeatedly eye-witnessed the “treatment” to be directly inducing the autoimmune diseases. Yet, they stubbornly refuse to believe their own eyes.
Very similarly for autism, there have now been tens of thousands of parents who have firsthand eye-witnessed vaccines destroying their children and causing autism. Many pediatricians have eye-witnessed it to happen too. This is a fact, and yet in the face of this overwhelming real-world evidence the so-called experts refuse even to consider it to be a possibility. They too stubbornly refuse to believe their own eyes.
Of course, with both autism and the autoimmune diseases, most physicians have absolutely no clue as to what’s causing the disease, no clue how to effectively treat it, and therefore no chance of curing it. So, these people are not the “experts” at all. Additionally, given their positions as physicians, and the public trust placed in them, their denials, and refusals to face the obvious facts completely disqualifies them to any claim of being the “experts.” It also completely disqualifies them from having any claim to being scientific. At best, given the gravity of the situation, their collective conduct is simply criminal negligence.
Now, in the context of real science, what intrigued me here was that the “light in the eye being lost” is a documented symptom of vitamin A toxicity, and so are seizures. And then seeing these same conditions occurring in kids shortly after they have been given a vaccination was a fascinating possible connection. But, the real connections are much deeper than just sounding similar. There’s a much deeper, and very scientifically plausible, connection here. It’s deep within the cell, and in our misunderstanding of immunity. It’s the potentially deadly combination of vaccines, and elevated serum and storage levels of vitamin-A, and its downstream metabolite, retinoic acid.
that are activated by vaccines?
It is now well understood that the immune system uses pathogen-associated molecular patterns (PAMPs) to activate pathogen-recognition receptors such as TLR, and also a host of other more recently discovered receptors: retinoic-acid inducible gene-based (RIG)-I like receptors, or RLRs, and cytosolic nucleotide oligomerization domain (NOD)-like receptors, or NLRs. These receptors bind various pathogen ligands … more.
By Stanley A. Plotkin, MD, Walter Orenstein, MD and Paul A. Offit, MD
ISBN: 978-1-4557-0090-5; Page 59
Oh, would you look at that, it’s a bunch of them, including the retinoic-acid ones. Somewhat paradoxically, these cells that have been damaged by the vaccine’s adjuvant, and that have not been completely killed by it, are now the much bigger concern. These cells are now going to start processing latent, and circulating retinol in serum, into retinoic acid. They are now little mini factories producing retinoic acid on a non-stop basis. This will continue for as long as these cells can stay alive. Additionally, I don’t really believe Plotkin’s and Orenstein’s determination that the so-called recently discovered receptors are simply being “activated.” No, I believe what’s really happened is that the cell’s membrane has been sufficiently damaged by the vaccine’s adjuvant to allow these other solvent based molecules to more easily pass through the cell’s otherwise protective fatty membrane. And that’s why there’s a whole “host of other” receptors that appear to be “activated” at the same time. Now, there are a few super, critically, important points to understand here. Firstly, how do they know that the retinoic acid receptors have been activated? It’s by measuring and detecting the increased quantities of retinoic acid in the cell’s nucleus and cytoplasm. So, what they’ve really detected is the increased rates of retinoic acid production, and from that increased rate they then infer that the “retinoic acid receptors” have been activated. The second important point to understand is that the overall process can cascade out of control. This fact has also been well known for decades now in the context of lung cancers; toxin damaged cells in the presence of more retinoids causes not only more incidences of the cancer, it also causes the cancers to accelerate.
In all three of these studies, taking very high doses of beta-carotene, with or without 25,000 IU retinyl palmitate or 325 mg aspirin, did not prevent lung cancer. In fact, both the CARET and ATBC studies showed a significant increase in lung cancer risk among study participants taking beta-carotene supplements or beta-carotene and retinyl palmitate supplements.
https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/
Thus, with that I think the connection is revealed. The vaccines are doing exactly what they are designed to do. Their adjuvants are breaking down cell membranes. As with the toxins released by tobacco smoking, the adjuvants, say such as the aluminum, etc. bind onto the cells outer membrane and vastly compromise its integrity by increasing its permeability to the retinoids. The compromised cell membranes effectively prop open the door so-to-speak and allow more circulating retinoids to quickly pass into the cell’s interior and then to be converted into retinoic acid.
This brings us to yet another crucially important bit of evidence that the pro-vaccine camp believes that they have on their side of the debate. That’s the fact that there are kids who have descended into autism, and that they have never been vaccinated. It’s like, Ah-ha, there you go, something else other than vaccines is causing autism. But, of course, this does not mean that vaccines are not causing autism too. Rather, it is clear evidence that vaccines are not causing all incidences of autism. More correctly, we can just say that vaccines are not acting alone in causing autism. Therefore, what’s far more logically plausible, is that vaccines are causing a changed cellular state that is then enabling a potential background toxicity condition to manifest itself. And, rather extraordinarily, that’s exactly what the adjuvants in the vaccines are designed to do! The adjuvants are cytotoxins that the designers of the vaccine have expressly included in the vaccine so that cellular damage occurs. Once damaged, how long could these poisoned cells be producing retinoic acid and defective, and thus immune alerting, proteins for? Well, maybe for about the next seven years!
Therefore, I think a good analogy for understanding how a small vaccine jab could cause such a devastating long-term disease such as autism is that of throwing a lit match into a forest. Depending on the underlying moisture conditions in the forest that lit match could be a completely harmless event or it could be a disastrous one. In the early spring, that lit match does nothing. Conversely, in late summer, or when the forest is dry, that one small lit match could lead to a ten-thousand-acre forest fire and burn down towns in its path. In my previous e-book, I’ve documented this cascading chain reaction in the context of if causing the autoimmune diseases and SIDS. But, of course it is not always going to be quick, or necessarily fatal. The process can happen more slowly, and be sustained over longer periods of time, even decades, leading to permanent brain damage.
Next, let’s further test the pro-vaccine camp’s claim of having science on their side. Let’s look at some of their real data, and do real science. The source data for this investigation is from the 1987 study:
Diphtheria-Tetanus-Pertussis Immunization and Sudden Infant Death Syndrome
ALEXANDER M. WALKER, MD, DRPH, HERSHEL JICK, MD, DAVID R. PERERA, MD, MPH, ROBERT S. THOMPSON, MD, AND THOMAS A. KNAUSS, MD, PHD
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1647245/pdf/amjph00259-0017.pdf
This study looks at the timeframe of reported SIDS deaths in correlation to the DTP vaccine. One of their important conclusions from the study is:
Focusing on very narrow time intervals following immunization, we found the SIDS mortality rate in the period zero to three days following DTP to be 7.3 times that in the period beginning 30 days after immunization (95 per cent confidence interval, 1.7 to 31).
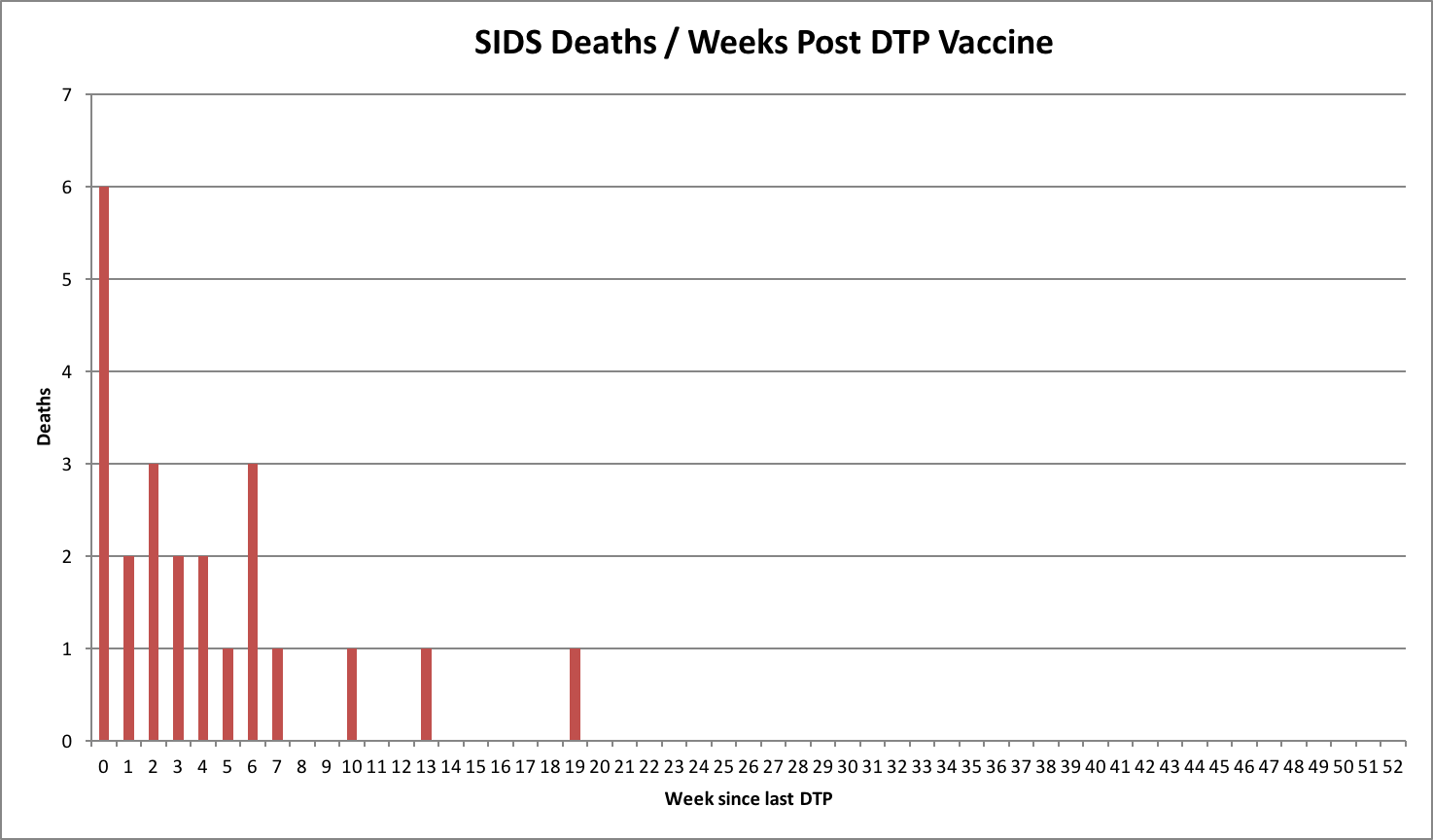
Figure 20 SIDS deaths in relation to date of recent DTP vaccination
|
I’ve plotted the report’s primary dataset in the chart shown at right.
Astonishingly, some of the SIDS deaths are on the same day of vaccination, and 65% of the deaths are within just two weeks of vaccinations, and a whopping 86% are within 4 weeks. Whereas, if there were no causal relationship here, we should not see this abrupt early clustering and expect to see a far more random distribution in the post 52 weeks, and therefore only about 4% and 8% of the SIDS deaths occurring in the same short two-to-four-week timeframe following vaccination. In other words, the rate of SIDS deaths should be far more spread-out and at least ten times lower in these first four weeks following vaccination. The probability of the SIDS deaths having randomly occurred in this pattern is less than about 4.96×10-33 – or if you prefer the decimal notation, it’s less than 0.00000000000000000000000000000000496.
Therefore, seeing the above chart it is simply impossible for any honest and legitimate scientist to not realize the obvious. The DTP has simply killed these infants, and the medical establishment has been covering it up by foisting the blame on the phantom SIDS label. The obvious conclusion that the DPT vaccine has indeed killed some infants in this study group is not lost on the authors of this report either.
Even if all the SIDS occurring within three days after immunization were due to DTP, immunization practice would not have accounted for more than about 10 percent of SIDS cases at GHC.
So, they appear to be saying, “oh, it’s OK, we’ve only killed 10% of them with the vaccine.” Except, why would they think that the responsibility for the killing magically stops on the third day post DTP? Additionally, what evidence do they have that it’s only 10% of the SIDS cases were caused by the vaccine? It’s none what so ever. Obviously, it’s just the opposite, and the DTP has most likely killed most of the SIDS victims in this study. The killing has been ongoing for the last thirty years too. Using the same SIDS ratio presented in the above referenced report, this means that the DTP vaccine has probably killed about 90,000 American infants over the last thirty years. Now, with that real science, how can anyone not have a major problem with that? Yes, to “protect” kids from infections, they’ve killed at least 90,000 of them, and of course they have injured hundreds of thousands of more kids too.
Additionally, with the vaccine companies, and the medical establishment, having had this knowledge for the last thirty years, they have silently stood by and allowed the killing to continue, and have thereby been complicit in it. Therefore, let’s be completely blunt about it. Their claim of having the science on their side is a conniving lie, and they’ve continued to commit the mass-murder of infants solely to protect their profits. Clearly, that’s just about as evil as it gets.
Next, we need to ask the other gigantic “what’s that elephant standing in the room” type question here. With their claim of being the esteemed experts in medical science, how is it possible the “experts” have not been able to determine the real cause of death in the now hundreds of thousands of SIDS cases? Seriously, how could’ve they possibly not been able to determine any cause of death in these infants? With that colossal failing, it’s rather obvious that they are not the experts at all. We need to realize that “SIDS” is just the place the vaccine industry hides the dead bodies of all the infants they’ve killed. No pediatrician, and no parent, should have ever accepted this “SIDS” label as being a legitimate cause of death. The fact is that the “SIDS” excuse is no more meaningful than saying that the Easter Bunny was the cause of death, because neither of them exist!
High serum serotonin in sudden infant death syndrome
Sudden infant death syndrome (SIDS), the leading cause of postneonatal infant mortality, is defined as the sudden death of an infant less than 1 y of age that remains unexplained after a complete autopsy and death scene investigation. Although SIDS has been associated with deficiencies in central (brainstem) serotonin (5-hydroxytryptamine, 5-HT), there are no known peripheral biomarkers for SIDS. Here we demonstrate increased serum serotonin levels in a subset (31%) of SIDS infants compared with control infants.
Proceedings of the National Academy of Sciences of the United States of America. 2017;114(29):7695-7700.
doi:10.1073/pnas.1617374114.
With this information, the first question we need to ask here is; what can cause this increased level of serotonin in serum? Not surprisingly, it’s retinoic acid.
13-cis-Retinoic acid alters intracellular serotonin, increases 5-HT1A receptor, and serotonin reuptake transporter levels in vitro.
In addition to their established role in nervous system development, vitamin A and related retinoids are emerging as regulators of adult brain function. Accutane (13-cis-retinoic acid, isotretinoin) treatment has been reported to increase depression in humans. Recently, we showed that chronic administration of 13-cis-retinoic acid (13-cis-RA) to adolescent male mice increased depression-related behaviors. Here, we have examined whether 13-cis-RA regulates components involved in serotonergic neurotransmission in vitro. We used the RN46A-B14 cell line, derived from rat embryonic raphe nuclei. This cell line synthesizes serotonin (5-hydroxytryptamine, 5-HT) and expresses the 5-HT(1A) receptor and the serotonin reuptake transporter (SERT).
...
Treatment with 13-cis-RA for 96 hrs increased the intracellular levels of 5-HT and tended to increase intra-cellular 5HIAA levels.
Issue published: October 1, 2007
https://doi.org/10.3181/0703-RM-83
Kally C. O’Reilly, Simon Trent, Sarah J. Bailey, 1, Michelle A. Lane, 1, 2
Institute of Cellular and Molecular Biology, The University of Texas at Austin, Austin, Texas 78712; Department of Pharmacy and Pharmacology, University of Bath, Bath, BA2 7AY UK; and Department of Human Ecology, Division of Nutritional Sciences, The University of Texas at Austin
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5530643/
Then, the next obvious question we need to ask is; what can cause an elevated level of retinoic acid in infants? It’s vaccines of course. So, now we have this direct chain of evidence:
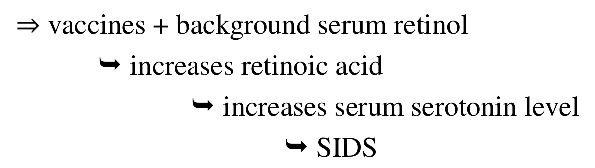
Seeing the elevated serum levels of serotonin in response to retinoic acid is hugely significant here. Our nervous system and brain are highly regulated by serotonin. Serotonin levels play an enormous role in our mood and our general sense of wellbeing. As a matter of fact, the role serotonin plays in the nervous system is so fundamental that its evolutionary history dates back more than 300 million years. And now, effectively suddenly, we have infant vaccines that abnormally alter these critical serotonin levels.
We also need to appreciate that infant deaths are just at the extreme end of the morbidity spectrum in response to the vaccine. Obviously, for most of the kids who were killed by the vaccine, it has taken about 2 to 4 weeks for their retinoic acid levels to build up and cause enough hypoxia and ischemic damage for the condition to become lethal. For many of the other kids who did survive the vaccination, they did not escape it unscathed. No, many of them most likely also suffered some degree of hypoxia induced damage too and were permanently, or nearly permanently, brain damaged by it. Obviously, on the extreme non-fatal end of that brain damage spectrum is autism.
The destructive retinol to retinoic acid oxygen depleting cascade is as follows:
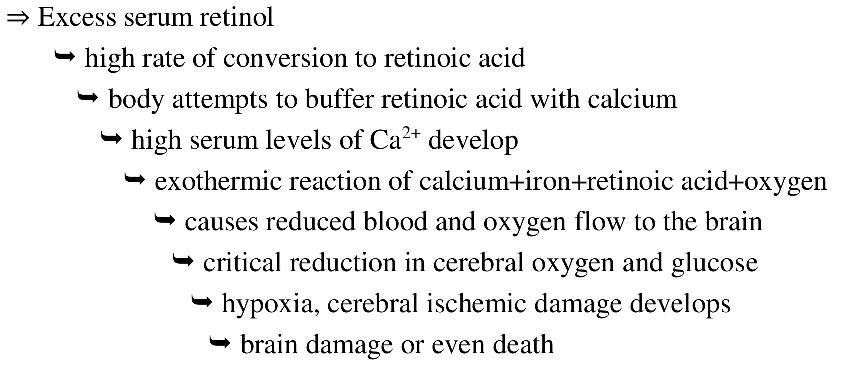
Quite surprisingly, even though hemoglobin is a huge protein molecule, C2952H4664O832N812S8Fe4, with something like 2,952 carbon atoms, it contains only 4 iron atoms. Therefore, any external factor that reacts with that iron will seriously compromise the blood’s ability to carry oxygen.
Here’s some interesting clinical evidence supporting this suspected connection between anemia and impaired CNS function.
Specific central nervous system processes (e.g., slower nerve conduction and impaired memory) appear to remain despite correction of the iron deficiency anemia. There is a general lack of specificity of effect and of information about which brain regions are adversely affected. Recent data from Chile showed a decreased nerve conduction velocity in response to an auditory signal in formerly iron-deficient anemic children despite hematologic repletion with oral iron therapy (Roncagliolo et al., 1998). This is strongly suggestive evidence for decreased myelination of nerve fibers, though other explanations could also exist. Current thinking about the impact of early iron deficiency anemia attributes some role for “functional isolation,” a paradigm in which the normal interaction between stimulation and learning from the physical and social environment is altered (Pollitt et al., 1993; Strupp and Levitsky, 1995).
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine. National Academy of Sciences.
ISBN 0-309-07279-4
So, it’s all subtly and yet directly interconnected. Of course, in addition to the nation’s infant formulas, low fat milk and other dairy sources being boosted up on vitamin-A, so too have the breakfast cereals in the USA. But, not only are those breakfast cereals spiked up with vitamin-A, many have had iron supplemented in to them also. The problem with that extra iron is that if it is not bound to hemoglobin it is not going to add to the transport of oxygen, rather it’s just the opposite, and it will scavenge oxygen.
Yes, it’s the perfect storm scenario being slowly piled up each morning with their breakfast. It’s like the forest drying out over the summer. All that’s needed for it to flare-up, and cause a massive oxygen consuming inflammation incident, is one spark. Quite likely, that spark is in their innocent looking vaccination. Additionally, maybe herein the following statement lies the explanation for why so many infants are now having seizures?
This is strongly suggestive evidence for decreased myelination of nerve fibers, though other explanations could also exist.
But, to many folks in the pro-vaccine camp, there can be no questioning of the other sacred cow of medical science, that of vitamin A being so beneficial. They’ll be able to cite studies that show that vitamin A “enhances” the immune response during vaccination. For example:
There is now substantive evidence emerging from animal and in vitro studies showing that VA and its metabolites have a powerful role in the regulation of immune responses. In particular, it has been shown that specific subsets of intestinal dendritic cells and macrophages are able to convert (vitamin A) VA into retinoic acid (RA) and that RA then enhances the induction of FoxP31 T regulatory cells (Tregs). In addition, Tregs induced by RA have a unique and highly specific tropism to the small intestine. Several studies have demonstrated that RA promotes Th2 and inhibits Th1 immune response pathways. Accumulating evidence now shows that a high concentration of RA can also suppress the generation of Th17 cells. Conversely, a recent study reported that RA at very low concentrations promotes Th17. RA may also regulate B cell proliferation and differentiation.
Landscape Analysis of Interactions between Nutrition and Vaccine Responses in Children
However, seeing the elevated conversion rates of retinol to retinoic acid in response to vaccinations should clearly be a huge cause for concern, and especially so during pregnancy. And, of course, seeing that retinoic acid “enhances” the production of T, and Th2 cells should not be assumed to be a good thing to have happen. Not at all, it is just clear evidence that more cellular damage has occurred and that then in turn has forced the immune system to be more aggressive in its response. Some researchers are now noticing that this “enhanced” immune system response to elevated levels of vitamin A combined with vaccination is causing serious harm.
VA (Vitamin A) and DTP/OPV (Oral Poliovirus) vaccines
Although overall mortality rate did not differ between the different dosing of VA, the authors reported that the lower dose was associated with significantly reduced mortality in girls only (mortality rate ratio, 95% CI ¼ 0.19, 0.06–0.66).
Source: As Above: Page 13S of 65S
And they go on to report other adverse reactions, but usually citing mortality rates as their primary measure of it.
VA and DTP/OPV vaccines cont.
After pooling results from these studies, they found a global mortality rate ratio for VAS compared with placebo of 3.06 (95% CI ¼ 1.00–9.38; P ¼ 0.03). Aaby et al. (5) also examined mortality data stratified by sex. They reported from the Bangladeshi study that female mortality was significantly higher than male mortality, especially in the group that received (Vitamin A Supplimentation) VAS with DTP vaccine. The female:male mortality ratio was 4.17 (95% CI ¼ 1.39–13.0; P ¼ 0.006) in children who received VA and DTP vaccines compared with 2.08 (95% CI ¼ 0.76–5.73; P ¼ 0.15) in those who received placebo and DTP vaccines, but the authors did not specify whether this difference was significant. Reanalyses from a study conducted in Navrongo (Ghana) also revealed that girls who received VA with DTP vaccine had a significantly higher mortality rate than girls who received placebo with DTP vaccine [mortality rate (95% CI) ¼ 2.60 (1.41–4.80)] (124). Their conclusion was that VAS interacted negatively with DTP vaccination in girls, but the authors did not provide suggestions on possible mechanisms that might explain these results.
Source: As Above: Page 13S-14S of 65S
VA and DTP/OPV vaccines cont.
The lower dose of VA was associated with a lower hospital case fatality in girls only but with a slightly higher morbidity (diarrhea, fever) in children aged 6–18 mo in either sex.
And …
Three other studies conducted in Bangladesh and Tanzania evaluated adverse events, but not mortality, after VA and DTP/OPV administrations. They all reported a significantly higher risk of bulging fontanelle, but no other serious side-effects, in children who received VA compared with those who did not.
And …
In 1 group, mothers were supplemented with 120 mg RE VA within 24 h of delivery and their infants received 15 mg with the 3 doses of DTP at 6, 10, and 14 wk of age and 30 mg at 9 mo of age. Mothers in the other group received 60 mg RE VA within 24 h of delivery and their infants received placebo with the 3 doses of DTP at 6, 10, and 14 wk of age and 30 mg RE VA at 9 mo of age. The study showed no differential beneficial effect of the high-dose VA on health outcomes. If anything, it rather indicated a detrimental effect of increased clinic attendances and poor gut integrity. None of the VA regimen was associated with bulging fontanelle, nausea, or irritability.
Source: As Above: Page 14S of 65S
Summary of findings
VAS (vitamin A supplementation) along with vaccination is associated with a higher risk of bulging fontanelle, which disappears rapidly and does not have short- or long-term health consequences (Table 6). It is also associated with a lower risk of diarrhea, but does not seem to have any effect on other adverse events. There is only weak evidence that VAS with BCG, DTP/OPV, or measles vaccination has an effect on subsequent mortality. The controversy regarding a potential detrimental effect of VA administered with DTP vaccines has led to considerable discussion in the literature and in specially convened meetings. The hypothesized negative interaction is biologically plausible, including the male-female difference.
Source: As Above: Page 15S of 65S
Obviously, there is a glaring inconsistency in this report between their earlier statements such as “girls who received VA with DTP vaccine had a significantly higher mortality rate than girls who received placebo with DTP vaccine” and then with their follow-on summary of findings claiming that “there is only weak evidence.” Except, let’s not forget that we are talking about the killing of a “significantly higher” number of children here. Maybe they missed the memo on this, but their criminal negligence causing bodily harm and death is a crime that is usually punishable by ten or more years in prison. Secondly, we need to seriously question their claims of there being no short- or long-term health consequences of bulging fontanelles. I’m sorry, but how can anyone think that seeing a child’s brain swell up with inflammation and bulge out of their skull is not going to have negative health consequences?
So, I’m not buying their hand waving excuse of “weak evidence” because here we have well-conducted, double-blind placebo-controlled, studies showing a direct connection between vitamin A levels, and the significantly higher rates of follow-on adverse reactions, including deaths, to vaccinations. Moreover, why would we think it’s limited to just the reported adverse reactions of bulging fontanelles (inflammation and swelling of the brain), poor gut integrity, and increased mortality rates? Then, let’s recall what food based substance is known to medical science that can even possibly cause the bulging fontanelle condition? Well, it’s vitamin A of course.
Hazard Identification
There are substantial data on the adverse effects of high vitamin A intakes. Acute toxicity is characterized by nausea, vomiting, headache, increased cerebrospinal fluid pressure, vertigo, blurred vision, muscular incoordination (Olson, 1983), and bulging fontanel in infants (Persson et al., 1965).
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine. National Academy of Sciences.
ISBN 0-309-07279-4
In addition to the above, since we now know that vaccines are inducing the natural conversion of latent vitamin A into retinoic acid and with the information from the WHO findings of: “abnormalities in CNS related performance (e.g. speech and language, and verbal IQ tests) from exposure to 13-cis-retinoic acid during the fetal period of development” that should pretty much close the loop on the theory aspect of this. Obviously, we need to broaden that scope of caused disease conditions and include middle ground conditions such as autism and other CNS damages too. We just need to drop the obfuscating psychiatric derived term of “autism”, and call it for what it really is. It is brain damage caused by the prolonged depletion of oxygen to the brain. What caused the prolonged depletion of oxygen event? A poisoning did.
It does not take a quantum leap of extrapolation to now conclude that autism is indeed a poisoning that can be induced by vaccines. And, there is no extrapolation at all required here to conclude vaccines are significantly harming and even killing many children. It’s simply proven in the above-referenced studies to be doing so. There’s no disputing it either, it is indeed happening, and acknowledged by existing research. Likewise, with the reported increase of intestinal dendritic cells producing more retinoic acid, and their observations of increased clinic attendances and poor gut integrity in response to vaccinations it should come as no surprise to see many kids diagnosed with autism present with a comorbidity of IBD.
Claims of a negative interaction between VAS and DTP vaccines leading to excess mortality in girls therefore warrant serious attention. Our view is that the proposed effects are biologically plausible but unproven. Although there are acknowledged limitations in the analyses that have generated the controversy, we support the view that the concerns warrant further investigation using appropriate and carefully designed studies.
Source: As Above: Page 20S of 65S
Here, in the above-referenced studies, the researchers are documenting the elevated risks of adverse reactions (and deaths) when vitamin A supplementation is just co-administered with vaccines.
Next, let’s analyze their position:
Our view is that the proposed effects are biologically plausible but unproven.
Source: As Above: Page 20S of 65S
The first half of the above statement is correct, but the second half regarding it being unproven is not. There has indeed been a well conducted, double blind, placebo-controlled study proving the increased, and adverse, immune reaction. It’s:
Men with Low Vitamin A Stores Respond Adequately to Primary Yellow Fever and Secondary Tetanus Toxoid Vaccination
Shaikh M. Ahmad, Marjorie J. Haskell, Ruhhana Raqib, and Charles B. Stephensen
Program in International and Community Nutrition, Department of Nutrition and USDA Western Human Nutrition Research Center, University of California Davis, CA 95616 and Immunology, Laboratory Sciences Division, International Centre for Diarrhoea] Disease Research, Bangladesh, Mohakhali 1212, Dhaka, Bangladesh, 2008
Quite astutely, the researchers who conducted the above study have identified not only the increase in the vaccine-immune response in the presence of higher background storage levels of vitamin A, they’ve raised the alert to it potentially inducing autoimmune diseases too. At least there are a few honest vaccine researchers who understand that “enhancing” the immune response to vaccines is not exactly safe, nor smart.
Some other honest researchers who have investigated the same issue state the concern more succinctly.
Though more complex, it is necessary to evaluate all health interventions in terms of their effect on overall mortality - and their potential interactions with other health interventions and potential sex-differential effects should always be investigated. Only in this way can we assure that the children in the poorest countries get the best possible treatment and avoid using large amounts of money and resources on interventions which may, in worst case, kill them.
Bandim Health Project, Statens Serum Institut, Copenhagen S, Denmark.
https://www.ncbi.nlm.nih.gov/pubmed/22239846
Next, we have the following astonishing study that also conclusively proves the vitamin A – toxicity connection with vaccines. It’s:
Neonatal vitamin A supplementation associated with a cluster of deaths and poor early growth in a randomised trial among low-birth-weight boys of vitamin A versus oral polio vaccine at birth
Results:
In the rainy season we detected a cluster of deaths in the VAS group and the trial was halted immediately with 232 boys enrolled. The VAS group had significantly higher mortality than the OPV0 group in the rainy season (HR: 9.91 (1.2380)). All deaths had had contact with the neonatal nursery; of seven VAS boys enrolled during one week in September, six died within two months of age, whereas only one died among the six boys receiving OPV (p = 0.05). Growth (weight and arm-circumference) in the VAS group was significantly worse until age 3 months.
Najaaraq Lund, Sofie Biering-Sørensen, Andreas Andersen, Ivan Monteiro, Luis Camala, Mathias Jul Jørgensen, Peter Aaby, and Christine Stabell Benn
http://www.biomedcentral.com/1471-2431/14/214
I have no doubt that these researchers had the very best intentions. However, they most certainly should not have been too surprised to see that a vitamin was somehow randomly killing these kids because for over the last four decades it has been documented to do just that. The only missing detail they need to now understand is that the vaccines are increasing the toxicity of that vitamin dose. None-the-less, as parents we can now say:
Our view is that the proposed effects are both biologically plausible and completely proven.
However, it is crucially important to understand that it’s not that the vitamin-A supplementation has “enhanced” the immune response to the vaccine, rather it is completely the opposite. It’s that the vaccine has “enhanced” the toxicity of the vitamin-A supplementation. It has therefore of course potentially “enhanced” the toxicity of any circulating and previously stored retinol too. Not surprisingly, and correspondingly, there are now thousands of North American parents who have indeed reported their children having developed autoimmune diseases shortly after vaccinations.
Additionally, unlike the kids in South East Asia, and Africa, our kids here in North America are at far greater risk with vaccines because they have been boosted up on extra vitamin A for most of their young lives and therefore have accumulated higher storage levels of it. Very unfortunately, many North American kids have had their retinol levels hugely boosted up too, and way past (by about 10×) anything that can be considered normal in the context of our human evolution. Obviously, with that, the presumed to be innocent vaccine is not so innocent anymore. As a matter of scientific fact, based on this new understanding of the vaccine’s adjuvant significantly increasing the toxicity of vitamin-A, no vaccine can be considered “safe”.
Moving along, what were the tangible actions that resulted from the so-called experts holding their “specially convened meetings” to discuss the “controversy” regarding a potential detrimental effect of vitamin-A administered with DTP? Did the “experts” warn parents of the significantly higher risks of having their kids being killed by the vaccines? Seriously, what have they been doing over the last ten years while more kids in this situation continued to be harmed and killed? Maybe they are still working on getting the wording of the worldwide press-release just right? Evidently, it’s rather difficult. Surely, they can’t just go with something straightforward, such as the following proposal:
|
Vaccines are now proven to be killing kids |
Now, you must be thinking that those super well-funded vaccine companies would have exhaustively studied and thoroughly understood the mechanism behind how aluminum adjuvants function before using them in our kid’s vaccines, right? Well, nope, of course not.
The development of aluminum salts (alum) as vaccine adjuvants was an empirical process with little understanding of the mechanism of action and, with decades of use, it has become clear that there is a need for alternatives where alum-based adjuvants are suboptimal.
Source: https://www.ncbi.nlm.nih.gov/pubmed/27718183
That’s correct, without even knowing how the aluminum adjuvants function, yet knowing full well that aluminum is a serious biological toxin, it has been used as one of the most common vaccine adjuvants for decades. How can anyone in the pro-vaccine camp keep a straight face and continue to claim to be the “experts” on vaccine science when they don’t have a clue about how one of the most important vaccine ingredients even functions? How can they claim that the “science is settled” when it has not even taken the most basic first steps in understanding it? Of course, the term “empirical process” really means by using trial-and-error techniques. So, therefore, by experimenting with various toxic substances they were looking for one that would really aggravate and piss-off the immune system. Of course, with little regard for long term safety, they found that the aluminum salts did the trick. And next, how should we interpret the statement “it has become clear that there is a need for alternatives where alum-based adjuvants are suboptimal?” To me, it sounds more like weasel words for “oh shit, we’ve screwed-up, and we now need to start over” and just maybe an unspoken “ooops, sorry about that kids.”
Based on this information, once again, their blanket claims of having science on their side are nothing more than a complete joke. These are mad-men who stupidly believe that we need to inject poisons into the human body to somehow make it healthier. They are simply frauds and imposters regarding “science” and it appears they have absolutely no respect what-so-ever for the human body.
The aluminum adjuvants are like tiny shrapnel filled grenades. When exploded into the injection site tissues the aluminum shrapnel embeds itself into the cellular membranes. And, of course, what these mad scientists did not consider is how extremely long-lasting that damage to cell membranes could be. That long-term damage to cell membranes then facilitates the accelerated and persistent conversion of serum transported retinol to retinoic acid. So, even though us parents are doing everything we can to keep our children safe and healthy, at the same time the vaccine companies have been somewhat secretly injecting them with well-known toxins that then facilitates this hidden long-term poisoning.
Next, we need to understand the great vaccine effectiveness mystery. What the vaccine industry uses to measure vaccine “effectiveness” is the vaccine’s ability to provoke the immune system into just building antibodies. Not surprisingly, what’s not used to measure effectiveness is the vaccine’s, or even the subsequently produced antibodies, ability to truly prevent infections. Of course, the ability to actually prevent infection would be a far more important and accurate measure of effectiveness. But, let’s just gloss over that little detail for now, and focus on something significantly more important. What’s super well known, and well documented, but a bit of a scientific mystery is that vaccine effectiveness is regional. That’s correct, the exact same vaccine administered in different regions of the world usually has drastically different effectiveness rates. For example, for most vaccines administered in the countries of the Western world, they have say about a 95% success rate in provoking antibody production. Whereas, in the developing countries, the effectiveness rate is usually far lower, say around 45%. It is also very age dependent, because in the younger kids the “success” rate in provoking antibody production can even be far lower, and often right down at 0% effective. So, the great mystery here is how can the exact same vaccine have such dramatically different outcomes? Of course, we know it’s not genetics because of the now vast genetic diversity in the North American population, and there are many people here now sharing the common ancestry with the people from the developing countries. There are of course some other theories offered as to explain the regional differences in vaccine effectiveness. None-the-less, what the vaccine manufactures are discovering is that if they first boost up the serum level of vitamin-A via capsule supplementation, they can significantly increase the effectiveness rates, and get the immune system to build the wanted antibodies. However, in doing so, as documented above, there’s this little glitch showing up, it’s that they end up killing an “excess” number of children, and causing an “excessive” increase in follow-on autoimmune diseases. But, the critically important evidence they are proving here is that if they can bring the vitamin-A serum levels up to being on par with that of North American kids, they can boost up the “effectiveness” rates to being on par with those in North America too, say around 95%. Obviously, with that, it should be clear that the reciprocal applies as well. That’s because our North American kids are already at or beyond being on par with the boosted-up vitamin-A serum levels. Clearly then, those exact same vaccines are causing an “excess” number of deaths and autoimmune diseases here too. Naturally, this matches perfectly with the material facts we are seeing on the ground. Yes, by their very own studies, they’ve now proven that their vaccines are killing and causing disease in an “excess” number of our children.
Additionally, we need to understand the second part of the mystery, and that is why is it, in both the developing countries and even in North America, that very young kids often don’t respond at all to vaccines. What’s observed, is that in many of these kids there is rarely an antibody development response. This lack of response is rationalized away by claiming that the infant immune system is just too undeveloped. But, that’s more complete fiction, and non-sense. What’s clear, in these pristine infants their serum levels of vitamin-A are just too low, and the vaccine’s adjuvant is subsequently not immediately damaging enough to alert the immune system into action. Of course, even knowing this information about a complete lack of vaccine response in the clear majority of newborns, the medical establishment, via the vaccine industry, is still insisting that parents need to vaccinate their kids on the first day of birth. Obviously, based upon this information, that practice should be regarded as complete insanity and its only possible purpose is revenue generation.
You might be thinking that a quick way to further test this overall theory in the context of autism is to measure the serum levels of retinol in autistic kids. Except, it’s not so quick. There are many, many factors at play here. Firstly, serum levels are notoriously bad at indicating storage levels.
It is important to note that the beneficial range of vitamin A exists within a narrow window and toxicity can be associated with both acute and chronic supplementation of vitamin A. Acute toxicity is readily assessed with the measurement of vitamin A levels in serum. Serum vitamin A measurement lacks sensitivity for the assessment of chronic toxicity because the vitamin A has increased overtime and is reflected in tissue stores rather than in serum.
Secondly, we’d need to know what their serum levels were at on the same day that they were given the vaccine. More importantly, we are not too concerned with serum retinol levels; rather it is the subsequent retinoic acid levels that we are really interested in. Additionally, with many cells having their retinoid receptors activated, they are now rapidly converting and depleting serum retinol levels. Therefore, I’d much more expect kids with autism to now have moderate to significantly lower than “normal” retinol serum levels, but with correspondingly somewhat higher levels of retinoic acid. Here are few reasons why:
Infectious diseases depress circulating retinol and contribute to vitamin-A depletion.” And especially so with measles.
Source: FAO/WHO expert consultation on human vitamin-And mineral requirements. Page 92
However, when considering the above statement, it is very important not to confuse cause-and-effect here. The vitamin A depletion may not have been caused directly by the measles virus, or the immune system directly fighting the virus. Rather, there’s a good possibility that the damage caused to the cell membrane by the measles virus allows more circulating retinol to pass into the cell and subsequently to be converted into retinoic acid. On a reasonable scale, this would be very beneficial in causing enough inflammation to kill off the virus. However, if there’s too much retinol (and likely so in older children), the rate of conversion to retinoic acid is going to be higher. But, if the body cannot buffer and neutralize that retinoic acid fast enough, it is going to be effectively the same as taking high-dose chemotherapy. Even more critically important to understand is that the process will start a chain reaction of cellular damage and cascade out of control by causing even more cellular damage. Of course, by not understanding this cascading process, doctors will diagnose this as emerging “autoimmune” diseases, allergies, anaphylactic shock, dry eye syndrome, and maybe, if they are brave enough, eventually even “autism.” Additionally, as I’ve documented in my previous eBook, there is a very unexpected beneficial consequence of kids getting the measles, or some other big infections. By getting the measles, with its significant drawdown on vitamin A stores, they are far less likely to encounter the autoimmune diseases, dementia, and even Alzheimer’s later in life. So, ironically, the measles virus and humans have been living in a somewhat symbiotic relationship for millions of years. This phenomenon is now being backed up in other research and it’s also an anecdotal observation made in The China Study. What’s documented in these studies is that in regions with high rates of chronic infections there is correspondingly virtually no diabetes, no heart disease, no stroke, no dementia, no Alzheimer’s and no autoimmune diseases, and much lower rates of cancer too.
A secondary reason why we should expect a lower than normal serum level of vitamin A in kids with autism is that the same phenomenon has been reported in the context of schizophrenia.
Mental patients. Specimens of blood were first obtained, over the period March 1951 - December 1952, from established patients of Claybury Hospital, a large psychiatric hospital in the London area. Most of these patients had been in the hospital for at least 2 years. Chronic schizophrenia accounted for more than 70% of the diagnoses; the others were subdivided between affective, obsessional or hysterical disorders, paranoid state, senile psychosis and mental deficiency. Most of these states overlapped, either with each other or with schizophrenia. The question soon arose, however, whether the low levels of vitamin A and carotenoids observed in these patients were associated with their mental illness, or with residence in the hospital.
By T. Moore and I. M. Sharman, Dunn Nutritional Laboratory
University of Cambridge and Medical Research Council
https://doi.org/10.1079/BJN19510015
I believe what’s happened in these patients is that they have some hidden cellular damage (possibly in the liver) that is allowing the vitamin A to be more readily converted into retinoic acid. Please recall that all the symptoms of schizophrenia are a match with those documented on the list of so called side-effects of taking Accutane.
Just as the exterior skin, and the internal epitheliums, is the body’s first line of immune defense from pathogen attack, we need to appreciate that the cell membrane is an important component of the immune structure. The cell’s membrane is the last line of immune defense. If a pathogen gets past the skin barrier and into the intercellular fluid, the various cells of the primary immune system can usually deal with it and take it out before it causes too much damage. However, once that pathogen, or the toxins it produces, passes through cell membranes, serious damage ensues.
Obviously, maintaining healthy and integral cell membranes is a critically important factor in a strong overall immune system. Dietary fats and proteins are key factors in maintaining the cell’s membrane. But, with vaccine adjuvants now containing metals, and even {tip content="Surfactants are compounds that lower the surface tension between two liquids, between a gas and a liquid, or between a liquid and a solid. Surfactants may act as detergents, wetting agents, emulsifiers, foaming agents, or dispersants."}surfactants{/tip}, that are specifically designed to attach to and damage cell membranes, the last line of immune defense has been seriously compromised. This will result in especially damaging cascading effects in the hepatic cells of the liver. So, although vaccines may have tricked the immune system into building antibodies to the vaccine’s targeted pathogen, they will have damaged a more critical and fundamental component of the immune system at the same time. After all, vaccines only give the immune system a head start in building antibodies. However, what the pharmaceutical industry has done is brainwashed people into believing that they are doomed if they encounter the natural virus without first being vaccinated. But, of course, that’s complete nonsense. For the most part, the vaccines don’t magically enable the immune system to build the needed antibodies. No, when presented with the pathogen in a natural way, the adaptive immune system is very capable of building the needed antibodies. Of course, our immune system has quite successfully, and naturally, been doing exactly that over say the last 10 million years of our evolution too. And, much more importantly, by building antibodies naturally the immune system is going to mount a defensive measure proportional to the incoming threat.
But, uniquely with vaccines, the immune compromising price the body pays to build the antibodies is exceptionally high. With the adjuvants, such as aluminum, phenol and mercury, now stuck onto, and getting jammed into cell membranes, a horrible and completely unnatural cellular damage scenario has occurred. This would have never, ever before occurred naturally over the last tens of millions of years of our evolution. The human body is not prepared for these toxins, or this damage condition. The toxins such as phenol, and mercury will of course cause immediate cellular damage. However, aluminum adjuvants will be mostly only damaging cell membranes, and in oily tissues such as the liver persist for decades. This is therefore a very plausible scenario to explain the new and silent emerging epidemic of hepatitis A infections.
So, for all the folks claiming that vaccines are “boosting” the immune system; no, they are not. They are damaging the immune system, and seriously weakening its very last line of defense. It is important to understand that the damaged cell membranes are not just allowing more circulating retinol to pass into the cell, and to then be converted into the highly toxic retinoic acid. They are now also allowing pathogens to more easily pass into the cell’s cytoplasm too! Therefore, vaccines are damaging the immune system and enabling more infections! To be very clear about this, it’s not inadvertent damage either. Invoking this damage is the express goal and purpose of the adjuvants that the vaccine designers need and want to have happen. This damage then causes the cells to produce the “Pathogen-Association Molecules” that are needed to bait the immune system into the fight. And to be extra clear about this, it is also not at all speculation. This adjuvant-damaging process is of course now well understood and well documented.24 In addition to the clinical evidence, there are now tens of thousands of parents who have firsthand eye-witnessed their kids develop eczema as a direct result of vaccinations. This is incredibly important supporting evidence, because these thousands of otherwise perfectly healthy kids did not suddenly dose up on vitamin A, and they did not suddenly overload their skin lipids with it either. Obviously, what’s happened is that it was some long-lasting cellular damage from the recent vaccine promoting and accelerating the conversion of stored and circulating retinol into the toxic retinoic acid form of the retinoid. That retinoic acid (and as clinically proven over the last 50 years in dermatology too) then moves into the sebaceous glands and causes the skin’s malformed structure, and its subsequent blistering damage, otherwise known as “eczema.”25 Want chronic infections? Eczema is a wide-open door for them. Therefore, very ironically, vaccines whose purpose is to protect kids from infections, are indeed causing other chronic infections by breaking down the skin’s all important barrier function.
24 http://www.invivogen.com/review-vaccine-adjuvants
25 https://youtu.be/giMd6VLZ-9Q
If the video has been removed from YouTube, click [HERE] to view a saved copy of this video in a popup window.
The above reveals the great vaccine irony. The more vaccines that you get over time the more susceptible you’ll become to all kinds of potential infections and even food based toxins, a.k.a., the autoimmune diseases. Since the damage to cell membranes can persist for seven or more years, the number of cells with adjuvant damaged cell membranes will just accumulate and offer substantially more easy attack vectors for all kinds of viruses and bacteria. This is also now being completely proven out in recent studies that show that people who get the flu vaccines are more susceptible to the flu, and colds, in subsequent years, than compared to people who don’t get the vaccine.26 Of course, exactly the same threat scenario applies to our kids. The more vaccines our kids get over time, the more susceptible they will be to all kinds of other infections, and even food based toxins too.27 Therefore, as a society, the more uptake we have on vaccines, the sicker we’ll become. Naturally, this is exactly what nature is demonstrating to happen. We, as a society, and especially our kids, are sicker than we’ve ever been before in the history of our nations.
Now, the administration of any vaccine during pregnancy is a very dangerous practice.
High dose vitamin A have a potent teratogenic effect and are therefore contra-indicated during pregnancy. Isotretinoin (retinoic acid) is responsible for a syndrome including malformations of the central nervous system, heart and thymus, together with craniofacial defects. The incidence rate is high and comparable to thalidomide (ie, 25%). This high teratogenic potency justifies a strict limitation of such a prescription in women susceptible to become pregnant.
PubMed – NCBI Arch Pediatr. 1997 Sep;4(9):867-74
https://www.ncbi.nlm.nih.gov/pubmed/9345570
With the incredibly well documented, and scientifically proven {tip content="Teratogenicity is the ability to cause defects in a developing fetus. It is a potential side effect of many drugs such as thalidomide."}teratogenicity{/tip} of any amount of retinoic acid during pregnancy (equivalent to that of thalidomide), and now knowing that vaccines will accelerate the conversion of circulating retinol into retinoic acid, no vaccine can be considered safe during pregnancy.
The effect of vitamin A status on IL-10 differed by vaccine and may depend on the underlying level and type of immune stimulation produced by the vaccine adjuvant. Because these changes in immune response correlated directly with liver vitamin A stores, it would be prudent to consider if such “enhancement” of immune function by high-level vitamin intake might increase the risk of inflammatory diseases in subjects with genetic or other environmental risk factors that affect immune function.
https://www.ncbi.https//naldc.nal.usda.gov/download/26258/PDF
And there’s ample amounts of evidence to show that many women in North America are already at borderline levels for serum levels of naturally forming isotretinoin just from their diet alone. Therefore, the potential extra spike in isotretinoin production resulting from any vaccine is incredibly dangerous. From the FDA’s warning on it we have:
CONTRAINDICATIONS AND WARNINGS: Accutane must not be used by females who are pregnant. Although not every fetus exposed to Accutane has resulted in a deformed child, there is an extremely high risk that a deformed infant can result if pregnancy occurs while taking Accutane in any amount even for short periods of time. Potentially any fetus exposed during pregnancy can be affected. Presently, there are no accurate means of determining, after Accutane exposure, which fetus has been affected and which fetus has not been affected.
Major human fetal abnormalities related to Accutane administration in females have been documented. There is an increased risk of spontaneous abortion. In addition, premature births have been reported.
Documented external abnormalities include: skull abnormality; ear abnormalities (including anotia, micropinna, small or absent external auditory canals); eye abnormalities (including microphthalmia), facial dysmorphia; cleft palate. Documented internal abnormalities include: CNS abnormalities (including cerebral abnormalities, cerebellar malformation, hydrocephalus, microcephaly, cranial nerve deficit); cardiovascular abnormalities; thymus gland abnormality; parathyroid hormone deficiency. In some cases death has occurred with certain of the abnormalities previously noted.
Cases of IQ scores less than 85 with or without obvious CNS abnormalities have also been reported.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2001/18662s44lbl.pdf
So, with that direct connection, is it any wonder why the USA now has one of the highest rates of birth defects in the world? Is it any wonder that the flu shot during pregnancy is now being linked with causing spontaneous abortions too? Of course, with this new information, it is now completely impossible to believe that any vaccine can be regarded as safe for infants too.
There are now multiple studies showing that children who have had an encounter with measles, and / or even the mumps, have a correspondingly lower likelihood of getting the childhood leukemias.
Support for an infectious etiology for childhood leukemia has also been derived from studies of early illness and common childhood infections. Although no one infectious agent has been identified, decreased risks of leukemia have been reported among children with prior measles, mumps, hepatitis A, and ear infections, as well as nonspecific viral infections.
Risk of Childhood Leukemia Associated with Vaccination, Infection, and Medication Use in Childhood: The Cross-Canada Childhood Leukemia Study,
American Journal of Epidemiology, Volume 167, Issue 5, 1 March 2008, Pages 598–606,
https://doi.org/10.1093/aje/kwm339
A similar protective effect is somewhat reported for early vaccinations too. The hypothesized etiology for this paradox is that the measles encounter (or the simulated disease challenge from vaccinations) has somehow primed up, or in some unexplainable way, improved their immune system function to protect them from leukemia. Not at all surprisingly, these Canadian researchers have also documented a strong correlation between younger infants who have been supplemented with vitamins and them subsequently having a significantly increased risk of developing the childhood leukemias. But, of course, leukemia is not an infection. Rather, it’s that stem cells have been driven into a bizarre and unnatural state of out of control rates of mitosis. Of course, we now know the chemical molecule that causes that exact behavior in stem cells.
So, there’s no need to over-think the etiology here. It’s rather clear that the measles infection has simply helped draw down the body’s vitamin A stores to non-toxic levels. Whereas, supplementing with vitamins has increased its storage levels. Clearly, in the youngest children with their correspondingly smaller liver volumes, and a massive number of fresh stem cells, the risk is rather high. Therefore, the childhood leukemias are just one more of the named diseases in the vast array of the possible disease consequences of vitamin A overload in infants. When you combine this information, with all the other (and what should be overwhelming) supporting evidence I’ve presented in my previous eBook, there can be no doubt as to the connection between vitamin A overload, and the childhood autoimmune diseases, cancers, and even SIDS. Of course, for the thought to be “protective” effects of vaccinations reported in the above-referenced study, it’s a very tricky balance. It’s tricky because it’s completely dependent on the infant’s current vitamin A storage levels, and their previous exposure to the horrible vitamin A palmitates (from infant milk formulas). If they can successfully buffer and eliminate the generated retinoic acid fast enough, then they might be okay. Otherwise, they will likely become profoundly sick and some will die from it.
So, for all the proponents of childhood measles vaccination claiming we need to protect kids at all costs from the dreaded disease, there are now a few surprising twists in the story. In the recent past, by allowing our kids to get the measles we were significantly protecting them from developing autoimmune diseases, brain diseases and psychiatric disorders, and even the childhood leukemias. And, quite contrary to the ridiculous fear promoting propaganda of measles being a deadly disease, the facts are that almost no one in North America dies from the measles itself. In the 1960s, and ’70s, millions of North American kids routinely got the measles, and the risk of death was exceedingly small, and no one felt even remotely terrorized by it. Rather, once again, it was completely the opposite, and measles was regarded as a nearly harmless nuisance type infection. Now, we’ve upset an important and hidden balance of nature. Measles was silently helping to keep our vitamin A stores in check. Except, now without getting a big infection there’s no external control of it over accumulating in early childhood. Consequently, the great tragedy here is that we now have at least a million kids in North America who have been permanently brain damaged by their vaccinations to supposedly “protect” them. Ironically, it was to “protect” them from what was a not only a pretty much harmless infection, it was an infection that would have really protected them from far more serious and longer-term diseases too.
Thus, it’s rather clear that we’ve traded off not-getting the short-term infectious diseases in exchange for getting the lifetime chronic diseases. The missing understanding is that high levels of vitamin A storage is a bit of a ticking time bomb. Of course, this is completely backed up by clinical measurements:
The average concentration of vitamin A in postmortem livers of American and Canadian adults is reported to range from 10 to as high as 1,400 μg/g liver (Furr et al., 1989; Hoppner et al.,1969; Mitchell et al., 1973; Raica et al., 1972; Schindler et al., 1988 Underwood et al., 1970). In developing countries where vitamin A deficiency is prevalent, the vitamin A concentration in liver biopsy samples is much lower (17 to 141 μg/g) (Abedin et al., 1976; Floresand de Araujo, 1984; Haskell et al., 1997; Olson, 1979; Suthutvoravoot and Olson, 1974).
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes,
Food and Nutrition Board, Institute of Medicine. National Academy of Sciences.
ISBN 0-309-07279-4
Yes, it’s affirmative, these people in the poorer nations who have about 10 times lower vitamin A stores in their livers also have at least 10 times lower rates of the chronic diseases.
There is yet another great unknown here with vaccinations. That unknown is whether a child has already naturally encountered the target virus much before the vaccine is administered and therefore the vaccine dose is then their second major exposure event. In this scenario, the child’s immune system will have already naturally prebuilt antibodies for the virus. Then, when injected with the vaccine, the already prepared body mounts an immediate and massive inflammatory response. It is not the normal gradual response the body would be mounting as it builds up its antibody arsenal directly proportional to the incoming threat. Moreover, since we know so little about immunity, we don’t know how the immune system gauges the threat. If there were only a few viruses slowly sneaking through say the epidermis, the immune system might very wisely mount a proportionately smaller response. However, by injecting a vaccine directly into the muscle and bloodstream, the virus or viral proteins are introduced much deeper into the body. In the view of the immune system, this deep injection and the immediate appearance of the virus might pose a much more alarming and graver second-threat scenario. Clearly, to the immune system, it appears that the outer breaches of the defenses (the skin) must have been broken open. Therefore, in that scenario, and with its prebuilt and ready antibodies, the immune system will very likely mount a much more aggressive response. The accelerated rate of that response could be catastrophic.
Another, and critically important, unknown here is the kid’s stress and anxiety level and what their emotional reaction to the vaccine injection itself is going to be. Why this is such an important factor is because the body will be starting to mount its Fight or Flight response28 initiating the Glycogenolysis Signaling Cascade.29
With quickly elevated stress levels, the liver is going to be releasing large amounts of glycogen and stored retinol into serum. This is the body’s standard response to a perceived serious threat because the body needs massive amounts of energy to be delivered into the muscles within fractions of a second.
Except now, with the vaccine’s cytotoxic adjuvant damaging cells, and activating cellular retinoid receptors at the same time, more retinol will be processed into retinoic acid too. However, it’s not just the few thousand cells that have had their retinoid receptors activated by the vaccine’s damaging adjuvant that will be converting retinol into retinoic acid. It is every cell in the body contributing to the process, that’s right every cell in the body can convert retinol into retinoic acid. That little discovery, made around 1987, should have been one of the biggest “oh shit!” moments in medical scientific history. Of course, this overall scenario of a blast of retinoic acid causing disease and death in children is in no way speculation. Nope, it has absolutely and definitely been proven, and it continues to be proven about 10,000 times over each year, and year after year too. It has been going on for the last four or five decades too. That’s correct, the vitamin-A supplementation programs going on in South East Asia provide us with the conclusive evidence that this is indeed happening.
This scenario of having massively high storage levels (or from capsules) of retinol quickly released into serum is completely abnormal in the context of human evolution. But, the Fight or Flight response initiating the glycogenolysis signaling cascade is absolutely normal, and fundamental to being human. This scenario also completely correlates with many people who report that their first encounter with autoimmune disease, and even cancer, occurred shortly after a period of sustained high stress.
28 http://learn.genetics.utah.edu/content/cells/fight_flight/
29 http://learn.genetics.utah.edu/content/cells/cellcom/play-by-play/
In addition to the 10,000+ eye-witnessed accounts, and the above referenced published scientific studies effectively proving it too, we now have the very specific and scientifically plausible explanation for how vaccines are causing autism. Therefore, yes, vaccines are causing autism. And, just in case any of the deniers to the modern-day Holocaust being inflicted upon our children happen to be reading this, and they still fail to understand the connection here, let me make it super simple with a trivial bit of predicate logic.
- Vaccines are proven to promote a dramatic increase in the body’s production of retinoic acid by damaging cell membranes.
- Retinoic acid is a highly toxic molecule that is proven to cause all the symptoms and comorbidity conditions of autism (including bulging fontanelles and chronic brain inflammation).
- Therefore, vaccines are now proven to be triggering and causing many of the cases of autism.
The only remaining question here is what are you going to do now? You can try to continue to hide behind the smoke screens of non-sense and fake science and BS excuses, and thereby knowingly continue to participate in harming and even the killing of children. Or, you can accept the science, and actively speak out about the now known dangers of vaccines.
To me, the science and technology behind most vaccines is so completely primitive, it’s almost Stone Age science. One of the primary reasons for me making that statement, is that just after a few minutes of thinking about it, it’s clear that the vaccines don’t actually need the cytotoxic adjuvants at all. The foundation of vaccine “science” is the current belief that with the cytotoxic adjuvants damaging or killing cells, the molecular artifacts of that destruction will bait the immune system into finding the vaccine’s target virus (or viral proteins). Basically, the science of vaccines is to put somewhat compromised live viruses, or bacteria, or fragments of them with well-known cytotoxins into solution, then inject it into people, and hope for the best. With the associated cellular damage caused by the cytotoxin, the immune system might then find and build antibodies to the targeted virus. Of course, they have no backup plans (other than BS excuses) for when things go wrong.
But, the vaccines don’t need to kill or damage cells at all. They only need to include the damage association molecules, or what Plotkin et al. call the pathogen associated molecular patterns (PAMPs). Using just PAMPs to bait the immune system into the fight would probably do the job and make vaccines vastly safer.
Here's a bit of a silly analogy to make the point about just how primitive the current science behind vaccines is. Imagine that you needed to test the smoke alarm in your home. To test the smoke alarm, you'd build a small campfire on the floor and light it. Then, once the smoke alarm was set off, you would frantically try to stomp out the fire. Most of the time, this technique would adequately test the smoke alarm. However, some of the times the fire would rage out of control and burn down your house. Of course, no one would do such a foolish thing to just test a smoke alarm. Obviously, we could simply use a small smoke canister to test the alarm.
Although that’s a bit of a silly analogy, there’s nothing humorous about the origin of the so-called science behind vaccines. What the pharmaceutical companies want you to believe is that vaccines are one of the greatest discoveries of medical science. But the origin of vaccines has nothing to do with science. It dates way back to the development of the smallpox vaccine. In the 1790s a madman named Edward Jenner scraped the pus from a blistering infected teat from a cow, put it in a wooden bucket, allowed it to fester and culture with thousands of other unknown bacteria, and then jabbed it into kids, calling the solution a “vaccine.” If anyone did this today, they’d be charged with bioweapons-terrorism. Yet, we are supposed to believe that’s the greatest discovery in medical science.
Of course, many, many of the kids who were injected with the so-called vaccine quickly became diseased and died from it. Moreover, and not surprisingly, the rates of smallpox increased in the towns that allowed such insanity to be practiced. Now, try not to laugh, but that’s the foundation of the wonderful, modern science of vaccines. And when you honestly and genuinely study the history of it, not much has changed since then. Additionally, when you discover that far less then 10% (and more likely even less than 1%) of Europeans in that era were ever vaccinated, the claim that the vaccine eradicated smallpox is nothing more than another absurd lie. Seriously, when you consider that there were about 200 million people living in Europe in the 1790s, it’s rather difficult to believe Jenner’s wooden bucket of pus was large enough to vaccinate even the tiniest fraction of all Europeans. Of course, there’s also no possibility that a handful of so-called physicians could have managed to vaccinate even one million people in that era. Additionally, with no refrigeration, it would have been impossible to preserve a viable bucket of vaccine (umm, festering pus). Therefore, claims that vaccines eradicated smallpox are just more absurd nonsense. Realistically, based upon these numbers, the entire premise of those claims is completely ludicrous.
The current scientific community behind and pushing vaccines has quite factually all the hallmarks of being a cult,30 and Edward Jenner is held up as the ancient high-priest of that cult. And just like some ancient Aztec religious cult sacrificing random children to appease the gods of disease, the modern-day cult a vaccine science is completely willing to do much the same thing today.
| Table 5 The Top Food Allergies in the USA | ||
| Food Allergies | Vaccine growth / carrier medium | |
| Eggs | Egg albumin | |
| Peanuts | Peanut oils | |
| Fish | Fish Oils | |
| Milk | Lactose | |
| Shellfish | Fish Oils | |
| Wheat | Gluten | |
There are many more reasons why we should consider vaccines as being primitive Stone Age science. The next biggest reason is the risk of vaccines being contaminated with foreign and food based proteins that the immune system may inadvertently build antibodies to, is also very high. The fact that vaccines are indeed causing many of the food allergies now showing up in our children is being repeatedly proven by the ultimate authority on science, nature itself, and therefore is clearly happening.
Here, in just the context of allergic reactions, vaccines are probably responsible for killing at least another 1,000 American kids each year just due to anaphylactic shock. We also now have about two million kids running around with a lifelong, and life-threatening dependency upon their epipens (epinephrine auto-injectors). What could have even possibly caused this massive increase in “allergies”, apparently completely out of the blue, and all of a sudden too? Logically, given the scale of it, there is only one plausible explanation. The immune system has been tricked into building antibodies to food proteins that were included as part of a “safe and effective” vaccination they’ve been given. The anticipated, and naively hoped for, immune response to the vaccination is that the immune system finds only the vaccine’s target viral proteins. But, there’s no guarantee of the process being that restrictive.
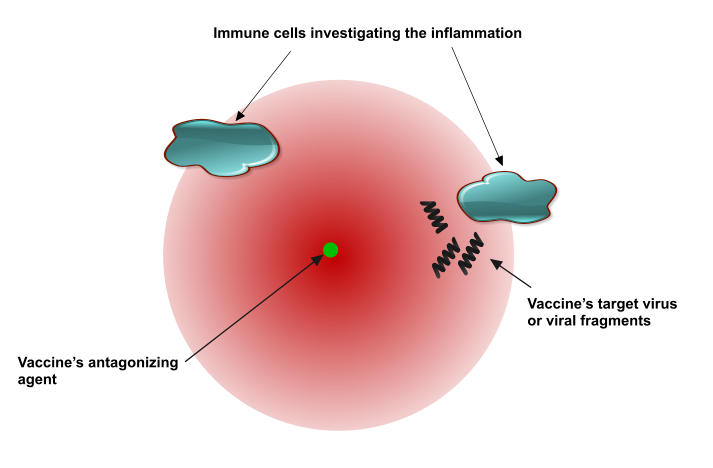
Figure 21 Immune cells investigating vaccine caused inflammation
|
No, not at all. To the immune system, now finding whole food proteins in the same vicinity, and immediately injected with the vaccine, and whole food proteins that would have never normally been found like this in muscle tissue, it tags it as being a possible antigen. It then builds antibodies against the food protein too. The kid has just been vaccinated against a food protein, and the medical experts simply call it a newly developed “allergy.”
However, for most people these vaccine-induced food “allergies” might not immediately show up. They may only show up years, or maybe even decades, later. They’ll most likely only show up when a compromised intestinal lining (leaky gut) allows more food proteins to directly enter the serum.31 Then, not only is the immune system going to be detecting whole food proteins in the serum that should not be there, it has already been tricked into associating these food proteins with having caused severe cellular damage. In addition to all of that, there is the risk of the vaccines being contaminated with animal proteins or even unbeknown viruses or even parasitic {tip content="Viroids are small infectious pathogens. They are composed solely of a short strand of circular, single-stranded RNA. Unlike viruses, they have no protein coating. All known viroids are inhabitants of angiosperms, and most cause diseases."}viroids{/tip} such as {tip content="Prions are misfolded proteins with the ability to transmit their misfolded shape onto normal variants of the same protein. They characterize several fatal and transmissible neurodegenerative diseases in humans and many other animals."}prions{/tip}.
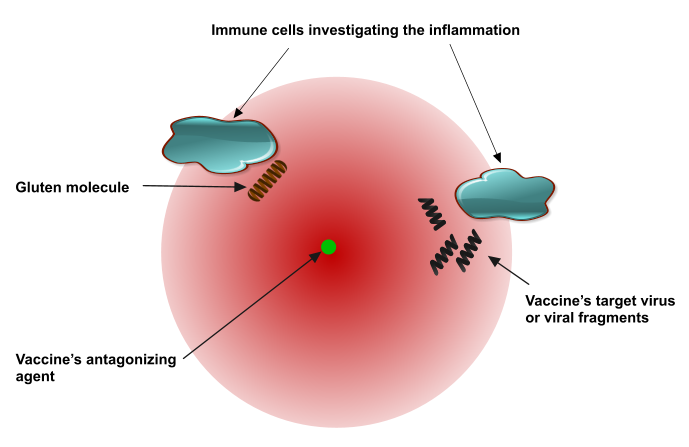
Figure 22 Immune cells finding a food protein included in the vaccine
|
Moreover, to call a vaccine a “medicine” is a complete misnomer. All vaccines contain serious toxins. Those toxins are in the vaccine for the express purpose of causing cellular damage and cell death. That damage is simply used to generate the damage association molecules that bait and trick the immune system into developing antibodies, and mostly antibodies that will never be needed. And, if by the time they are needed, they could be nullified. That’s not science, it’s primitive and foolish. Likewise, the notion of “herd immunity” has no basis in science, and there’s not a shred of evidence to support it. When you think about it for even just a few minutes, it’s completely ridiculous. Just one of the reasons why it’s such a ridiculous notion is that vaccines have never prevented a single person from getting an infectious microbe on the surface of their skin. No, even vaccinated people can still get the infection, the only difference is they’re able to deal with it more quickly and therefore might only carry the disease-causing microbes for a matter of days rather than a matter of weeks. Therefore, even vaccinated people are just as capable of being disease transfer agents. Thus, vaccines in no way, prevent the spread and transfer of disease. Even more ironically, people who have been given the live virus version of the vaccine, have been deliberately infected with it and are now direct transfer agent threats. The logical holes and flaws in the herd immunity argument are so gigantic you could drive a big yellow school bus through them.
31 http://www.thedoctorwithin.com/allergies/vaccines-and-the-peanut-allergy-epidemic/
The primary argument used to promote the need for developing herd immunity in the community is the need to protect the immune-compromised child. Except, even just the most basic premise here is absurd. The argument is that to possibly “protect” a few children, we need to force all other healthy children to be put at risk, including the risk of severe brain injury and even death. That’s right; we are told that to protect the few, we need to risk the many. How is that justifiable?
But, that’s just the starting point of the hypocrisy and absurdity of the ridiculous bullshit being propagated on us. The most powerful evidence demonstrating just how absurd the whole notion of herd immunity is the actual current vaccination practices itself. Here in Canada, kids are routinely vaccinated in their schools. So, for example, say we have 32 kids in a classroom, and two of them are immune-compromised and therefore are deemed to be too immune weak to be vaccinated. In this standard scenario, what happens on vaccination day, is that the 30 healthy kids are briefly taken out of the classroom, given the vaccine, let’s say the MMR, a live measles and mumps vaccine, and then sent immediately back into the classroom where they can interact with the two immune-compromised kids. Therefore, before vaccination the infection risk scenario in the classroom looks like this:
And then one-hour post vaccination it looks more like this:
That’s right, the 30 kids are injected with live viruses, and they are viruses that are transferable via air, and then immediately sent back into the classroom to interact with the so-called highly vulnerable immunosuppressed kids. If physicians are so concerned about protecting immunosuppressed kids, then this standard practice is complete lunacy! Because, for the freshly vaccinated kids, it will take several weeks for them to develop antibodies and clear the vaccine's virus. In the interim they are now direct transfer agents and shedding the live viruses. Therefore, what would need to happen to protect the immunosuppressed kids is to take them out of the classroom and keep them out for about 4 to 6 weeks’ post-vaccination day. They should be quarantined in their homes, and not at all exposed to the live-virus vaccinated kids.
But, of course, just keeping them away from the freshly vaccinated kids would not be sufficient either. No, they need to be sequestered off from the entire outside world too. That’s right, to adequately protect them they’d need to be not ever again exposed to playgrounds, public transit, grocery stores, libraries, restaurants, movie theatres, swimming pools, and any public places at all. But, the real clincher is that they can’t be exposed to any adults either. Not teachers, not babysitters, not aunts, uncles or grandparents, and not even their parents too because any of these adults can and will be carriers of live viruses. The real question completely ignored here is why these kids are immunosuppressed in the first place? Let me assure you that it’s not because of some lame “bad-luck” excuse. Rather, it’s because they’ve been poisoned, and for many of them that poisoning has come from a previous round of vaccinations too.
The concept of heard immunity is completely ridiculous, it’s a sham, a fraud and nothing more than fear promoting propaganda. It’s not only ridiculous, it’s offensive. We, are not a herd of animals to be managed as part of some grand farming operation. That’s the same view the Nazi doctors held for the people of the world, and I for one don’t appreciate the connotation of it.
If the modern day pro-vaccine doctors want to treat us as a herd of animals, then I suggest we round up the entire “herd” of all these doctors and vaccinate them for stupidity. Except, you might think there’s no vaccine against stupidity. But, oh yes there is. Let’s give them each 100 doses of the MMR vaccine, and all in one shot. After all, if they are so adamant and want to stick to the blanket claim that vaccines are safe and effective, then they should have no problem whatsoever in rolling up their sleeves and proving it on themselves. If we made this prove-it-on-yourself test a requirement for all doctors who want to continue forced vaccinations, the practice would come to an immediate screeching halt.
Now that we’ve jacked up our nations kid’s vitamin-A storage levels, and having this, not just plausible but, effectively proven scientific explanation as to how vaccines are causing prolonged disease, including the autoimmune diseases and autism, we need to be very cautious about how we proceed with vaccines. Although the threat for the more common serious infections such as measles and pertussis has most certainly not gone away, vaccinating kids for them is potentially far more damaging. We simply don’t know who is going to react and to what level of severity. But, we do now have a bit more information and parents can be more informed and weigh the pros and cons of it. However, tricking the immune system into developing tens, or hundreds, of different antibodies to virtually nonexistent threats is definitely playing with fire. The real mechanisms of that fire are currently something that we have almost no solid scientific understanding of. Therefore, with all the known huge risks, and major unknowns as to who’s vulnerable to them, I view the vastly widened vaccine schedule being forced on unsuspecting parents and their trusting children is simply more poisoning for profits. And, of course, the real “receptors” fully activated by the vaccines are the cash receptors in the back pockets of the pro-vaccine medical community.
Next, let’s question if “the science is settled” on vaccines, then why do we have this new discovery of the retinoic acid receptors being activated? Why do we have these other new discoveries of the amplifying effects of stored and circulating retinol and retinoic acid when combined with vaccinations causing deaths? Why do we have the new discovery of the intestinal dendritic cells processing more retinol into retinoic acid post vaccinations? Why, if they already know all there is to know about vaccine science, do we have this astonishing statement?
Randomized controlled trials investigating child survival according to several vaccine formulations and/or immunization schedules, with or without nutrient supplementation (in particular VA), are now justified.
Landscape Analysis of Interactions between Nutrition and Vaccine Responses in Children
Page 12S of 65S
The real question they are now needing to answer here is, why the hell are our safe and effective vaccines killing so many kids when administered with vitamin-A?
Therefore, no, the “science” of vaccines is not even close to being settled. Rather clearly, it’s primitive and we are just getting started with it. And, some more nearly useless randomized controlled trials (that will kill more kids) are not needed. What’s needed is just good old-fashioned thinking, and the ability to honestly see the basic facts that they are looking at. The first fact is that vaccines are indeed killing an “excess” number of children, and especially so when administered with vitamin-A. It’s a scientific fact, because nature is proving it to happen. The answer to the above question, and the only other little scientific fact that they’ll need to come to terms with, is that vitamin-A is not a vitamin at all!
Lastly, who the hell do we think we are kidding with the vaccines in the first place. Do we really think we’ll be able to keep ahead of the evolution of viruses in nature? No, we will not. It is a ridiculous and foolish notion pulled out of La La Land. Our best long-term defense against viruses, and other infectious disease, is maintaining strong, perfectly well structured epithelial tissues and cellular membranes. Ironically, the best chemicals known to modern science to destroy these protective tissues is the ones governments have supplemented into our foods and vaccines; yes, it’s vitamin-A combined with the aluminum adjuvants.
There is another great irony in this vaccine story. Nineteen years ago, when Andrew Wakefield first suggested a possible association between the MMR vaccine and autism he was attacked, called a fraud, vilified, ridiculed, and had his career destroyed. This attack was mostly from the medical establishment who claimed to have “science” on their side. However, what Andrew Wakefield did was incredibly fundamental to science. What he did was the most basic starting point in all scientific investigation and discovery. Andrew Wakefield simply made an observation. He saw an anomaly and a possible pattern in it. Even though autism was not at all in his field of expertise, he was curious. He started looking for more clues. This is the same behavior that every science teacher in America should be teaching all their students to have. Although, I highly doubt it will ever happen, I hope that someday Andrew Wakefield will be held up as a role model for future science students. The greatest tragedy in all of this is that there are now hundreds of thousands of children who have had their lives destroyed. We’ve also lost twenty years of progress in making real scientific discoveries into better understanding infectious disease.
Now, regarding Andrew Wakefield’s famous fraudulent study, I did something that I suspect the great majority of the folks in the pro-vaccine camp have not even considered doing. I took the time to read it. I very carefully read every single word of it. Not only is there no “fraud” in Wakefield’s report, there’s really no possibility of fraud in it. He does not present any data other than the results of lab tests, and of course there are no charts with missing axis labels, no charts mysteriously scrunched down using log scales. What Wakefield, and his co-authors, presents are the short histories of twelve cases; mostly based upon the accounts from their parents. He simply listens to what the parents of the kids are telling him, and reports a possible temporal relationship and suggests that it needs more investigation.
We did not prove an association between measles, mumps, and rubella vaccine and the syndrome described. Virological studies are underway that may help to resolve this issue.
Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children
A J Wakefield, et al.
THE LANCET • Vol 351 • February 28, 1998
He simply wants to be cautious, and to find out more. Of course, his real crime is that he’s dared to question the safety of vaccines. It’s interesting to note that when the so-called pro-science camp start attacking Wakefield they don’t attack or challenge his science, rather they attack him personally; they attack the man. They have no interest in honestly pursuing the truth. So, that’s not science, it’s more like street thug politics. The other tremendously sick irony here is that the real fraud being committed on vaccine safety research was going on at the CDC at about the same time that Wakefield was being accused and persecuted for it.32 And, the cover-up gets far worse. Wakefield, wanting to be cautious, had the hypothesis that the combined single shot MMR vaccine might be a bit riskier than giving the individual mumps, measles, and rubella vaccines over a slightly longer timeframe. Obviously, he suspected that the potential for vaccine harm was dose related. There would have been absolutely no risk what-so-ever to the public in following this suggestion. But, the response from the government regulatory agency, and the vaccine manufacturer to that suggestion was to nearly immediately pull the independent vaccines from the market. They took that potentially safer option away from parents. So, why on earth would they do that? I think it is obvious that they knew full well what the potential outcome of that modified schedule would have been. Very likely there would have been a correspondingly measureable drop in the rates of autism and other adverse vaccine reactions. Naturally, that bit of new data would have then significantly established the link between vaccines and autism. So, no, that potential new evidence could not be allowed to surface. It appears that they’d rather go on damaging and destroying the lives of children than to have the truth revealed.
In keeping with the well-established practices of a cult, what the medical establishment wants to do is to vulcanize the us-versus-them mentality within their followers. To do so they use Wakefield as a target to symbolize the evil “anti-vaxxers” that threatens the greater good of society (umm, their profits). As much as possible, they want to pin the sole blame for the entire anti-vaccine movement on this one man and this one study.
Of course, what they don’t want you to know is that it is in no way just Andrew Wakefield and this one study raising the alarm. What they don’t want you to know is that it’s hundreds of thousands of parents who have eyewitnessed the vaccine damaging event happening in their precious children. Even more importantly, what they also don’t want you to know is that the so-called evil “anti-vaxxers” do not even exist. That’s right, almost every single one of these parents were very much “pro-vaccine” right up until they witnessed their kids being seriously harmed after they had them vaccinated. Hiding behind their elitist claim of having a special and exalted status of having a monopoly on science, what the medical establishment wants you to believe is that the anti-vaxxers are somehow all uneducated, unscientific, and being profoundly foolish to not vaccinate their children.
Of course, what they don’t want you to realize is that it is exactly the opposite. What the anti-vaxxers are doing is incredibly scientific and being incredibly smart. To be a true scientist and to be truly smart you need to update your beliefs based on new evidence, and do so whenever that new evidence comes along. Genuine and smart scientists do this no matter how uncomfortable it might be to the established orthodoxy. In mathematics, this is called applying {tip content="In probability theory and statistics, Bayes' theorem, describes the probability of an event, based on prior knowledge of conditions that might be related to the event. For example, if the risk of developing health problems is known to increase with age, Bayes' theorem allows the risk to an individual of a known age to be assessed more accurately (by conditioning it on their age) than simply assuming that the individual is typical of the population as a whole."}Bayes’ theorem{/tip}. Yes, smart people, scientific people, update what they believe to be true based on new and compelling evidence and that is exactly what the anti-vaxxers are doing. That makes them pro-science. Therefore, the “anti-vaxxers” are simply now the vaccine educated.
More importantly, what the medical establishment does not want people to realize is that there isn’t even truly an us-versus-them divide between the two camps. That’s because what all the parents in both the pro-vaxxers and the supposed anti-vaxxers camps want is exactly the same goal. All of these parents simply want healthy and safe children. The only difference is that the vaccine industry has very deceitfully, yet thoroughly, programmed people into believing that the only way to achieve that goal is via vaccination. However, we can very quickly test that theory, and test it completely by asking one simple question. How’s has that vaccination program panned out in the real-world health outcomes of our children? The honest and real-world answer they don’t want you to realize is that it’s been a colossal disaster. Our children are now the sickest in the world, and they are the sickest they have ever been in our history. This gap is not just by a wide margin, but sometimes even by orders of magnitude too. Nearly one in two children now have a diagnosed autoimmune disease. A huge number of our nation’s children now suffer from depression, anxiety and other very serious neurological disorders. The USA now has the highest rate of preterm births, spontaneous abortions, birth defects, childhood cancers, and SIDS in the world, and by far too when compared to the underdeveloped countries. Additionally, our older children are near dead last in academic performance, whereas in the late 1960s they were in first place. Lastly, and very ironically, our children are now plagued with reoccurring and very difficult to treat infections too. Yes, the great quest to make our children healthy via vaccination has resulted in them having more infection and disease than in any other population of children on the planet. By any measure, the vastly widened vaccine schedule, when honestly considered in this larger context of real-world health outcomes has been a gigantic failure.
Of course, I’ve included the reference to Andrew Wakefield and the above discussion for a specific reason here. Quite unfortunately, when Wakefield pursues his follow-up investigation of the syndrome he and his co-authors have described; Wakefield suspects that the vaccines have introduced a hidden virus into the patients. But, it’s not a virus. The key giveaway is that the patients sustain a prolonged and chronic disease condition. This condition means there is a protracted chronic poisoning occurring. However, the investigation by Wakefield and his co-authors is in no way in vain. The cold case can very much be resurrected and easily reopened. What needs to happen is the comparison of the novel nodular intestinal hyperplasia documented in the Wakefield study with that documented by other physicians who have already investigated the novel nodular intestinal hyperplasia induced in teenagers who have been treated with Accutane for acne. I do not doubt that the striking similarities in these tissues will reveal the smoking gun: retinoic acid.
At the time of writing this, I’ve never met, nor spoken with Andrew Wakefield.
In the next chapter, we are going to have a deeper look into the state of scientific fraud within medical science. It is an almost unbelievably deep and dark rat hole.
32 CDC intentionally destroyed documents relating to Vaccines causing Autism. https://www.youtube.com/watch?v=68AYtcwg9rw
[ed. note: YouTube has removed this video. Link is to a Jan. 2021 report about this at Sharyl Attkisson | Untouchable subjects. Fearless, nonpartisan reporting.]
About two years ago, I had a conversation with my young 11-year-old nephew. He asked me how I was doing with my new “disease.” The conversation went something like this.
| Me: | “I am not too concerned. I’ve just gotten too much of a certain chemical in my skin, and it’s going to take some time to recover from it.” |
I went on to explain my theory about it like so:
| Me: | “There’s a chemical in certain foods that will slowly accumulate in the body. If you accumulate too much of it, it will make you sick. It’s kind of like filling up a water balloon. Imagine if water were toxic. If you filled up the balloon and all the water went inside the balloon, it would be perfectly safe. But, some of the times when you’re filling up a balloon, you fill it up too fast, and some of the water leaks out, and you have a small mess. If you really overdo it, the balloon might burst, and then you have a much bigger mess. And, well, I really over did it.” |
| Nephew: | “Do doctors know about this chemical?” |
| Me: | “Oh, yes. They do know all about it.” |
| Nephew: | Rolls his eyes, lets out a small scoffing poof of breath, and states: “Well, then you are wrong. Even I could figure that one out, and there’s no way all those smart doctors aren’t figuring it out.” |
Well, you’d most certainly think so. And, yes, it is just rather obvious. Yet, if it is rather obvious that the slow accumulation of vitamin-A will cause chronic disease, and the chronic diseases are in actuallity chronic poisonings, and their symptoms are a perfect match for vitamin-A toxicity, then why isn’t the wider medical community “getting it?” Not only are they not getting it, or seeing it, it appears that some folks are doing everything they can to cover it up and conceal it. However, probably one of the biggest factors in why they are not getting it is in their naïve belief in the infallibility of science. But, I think an equally big reason is rooted in the systemic scientific fraud in medical research. Once we understand this fraud, and the motivations behind it, I think we’ll have a clearer picture as to why they are not “getting it.”
One of the most surprising aspects of my investigation was the blatant scientific fraud showing up in much of the so-called medical research and peer-reviewed studies. And, no, I was not on the lookout for it. It was pretty much just jumping off the page at me. It’s not well concealed, and it’s not really hidden. It is blatant, in your face, plain as day stuff.
I was thinking, okay, maybe I had just stumbled into a particularly bad segment of the medical, scientific research. Or, maybe I had an advantage by being an outsider. Being an outsider, I was not slowly conditioned and acclimatized into this field of so-called science that needs to continually lie and falsify evidence. Maybe since I had no financial interests in any of this, I was not biased in my observations. I was fresh on the scene, and I was just looking at and seeing the naked plain facts.
But, whatever the reason, there it was, in black and white, in plain sight, no doubt about it, absolute and blatant scientific fraud. It was in the Accutane cover-up “study,” it was in the rebuttal “study” to Rothman’s birth defects report, it was blatantly obvious in the vitamin-A palmitate cancer causation cover-up “study,” it was in the vaccine so-called “placebo” studies. These are not minor frauds either. They are frauds of epic proportions, ultimately deeply affecting the lives of millions of people. The significance of what was being covered up in these frauds cannot be over stated. It is millions, and millions of people having their lives destroyed, and many of them being put into early deaths. Seeing fraud like this, on this scale, was rather damn shocking. But, I am not naïve. You’d almost expect to see frauds in highly contentious areas, such as vaccines. However, what truly surprised me was that some of these frauds were protecting a molecule. I kept asking myself, why are they protecting a molecule? Of course, this one molecule is a huge money maker just on its own, when sold as a vitamin supplement, and when sold as an acne, or chemotherapy drug. In these markets, this might account for say a mere ten billion dollars per year. However, once you understand that the subtle overdose of vitamin-A is in reality what’s making most people in the Western world sick, the equation changes. Now, we are not talking about just mere billions. It’s more likely north of a trillion dollars per year.
The great epiphany for me in all my research was that people do not normally get chronic disease. It is in no way normal for people to get sick like this, and with the rates we have in North America so far beyond normal, it proves it is not normal in the human population, like at all. The real normal is far closer to zero. Likewise, the same goes for cancers. Cancer rates in 1860 in Western Europe were around 1 in 10,000.33 But now in North America the life time incidence rates are nearly 1 in 2 for men, and 1 in 3 for women.
Why would the body self-destruct, when it’s normal function is to perpetually attempt to heal itself and remain healthy? Chronic disease just violates the laws of biology and nature. I know that sounds trite and simplistic, but once you really think about it, it is incredibly important. The only way for the human body to get chronically sick (other than infections) is to be either chronically poisoned or starved. Yet, not only is the medical establishment, and the AMA telling us the root cause of disease is “bad luck,” the AMA has decreed that food does not cause disease, nor can it heal disease. The FDA has legislated that only an “official drug” can be used to treat or heal a disease. But, chronic disease is not “bad luck”; that excuse is not only ridiculous, it is simply impossible when you look at the numbers. Of course, the “official drugs” are useless, because we don’t have drug deficiencies’, we’ve been poisoned.
But, if I can figure that out, so can many other people. Could this possibly be true? Sadly, not only is it possible, it is more than likely. Of course, if you know that people don’t normally get sick, and in a properly fed population, people won’t get chronically sick, then you can’t sell them drugs. People won’t buy drugs because they simply won’t need them. So, what do you do if your business is to sell drugs and people won’t and don’t normally get chronically sick? Of course, you make sure they get ample amounts of the “good stuff.” Just like they did with their lab rats. They knew exactly what to do. After all, how could anyone be deficient in a so-called vitamin that is found in nearly all normal foods. Additionally, if you’ve just gotten a patent on the synthetic manufacturing process of the said to be vitamin, how would you trick the general public and politicians into believing that they need to supplement with it. Well, you’d terrorize them with fear of course. What could instill such fear in the masses? How about financing some rigged experiments to “prove” that they will all quickly go blind without getting enough of it? But, more fantastically, as people slowly start getting sick due to its toxicity, you’ll sell them no end of other “drugs” to treat their new never-ending illnesses. It’s perfect. Clearly, North America is well on its way to becoming Disease Incorporated, and business is booming.
However, for the great majority of medical professionals, they are not complicit in this, at all. For many of the medical professionals working in the fields of the autoimmune diseases, or the chronic brain diseases, they have simply been misled in to believing these diseases are caused by mysterious, and unknown circumstances. Given the structure of the medical systems, they have had little choice but to buy into the pharmaceutical promoting studies. But, I’ve got to believe that many of them are at least aware of, and somewhat realize the corruption taking place right under their noses. Of course, for most of them, they don’t dare start asking too many questions or poking around into dark rooms looking for the real truths. No, that would almost be like biting the hand that feeds them. Therefore, to cling to the claim of being the experts in the field, they need to play along, and when dealing with patients, they continue to put on the guise of sophistication, and of having superior knowledge and expertise. In order to do so, they need to hide behind and support the bogus reports and fraudulent studies. After all, since they have no clue as to what’s really causing these diseases and therefore they then have no hope of doing anything meaningful for a patient without the pharmaceuticals. Without the pharmaceuticals, a physician has absolutely nothing they can offer a patient with an autoimmune disease or for most cancers. The only tool these physicians have in their “fix-it” toolkit is their prescription pad. Without that prescription pad, they are simply out of business. So, they know who’s buttering their bread so to speak, and they don’t want it quickly turned into burnt toast.
What I’ve seen in some of the medical “studies,” with profoundly negative repercussions for the public health, is indeed lies. It reads more like propaganda to promote the current system than being legitimate scientific research. So often in reports that discuss particular drugs, the so-called side-effects are hugely downplayed, minimized, and termed to be “mild.” For example, in the case of isotretinoin (Accutane, et al.) the symptoms of brain tumors, permanent damage to the eyes and vision, brain damage resulting in a permanent drop in IQ, and even suicide is termed “mild side-effects.” Not only is that such an egregious load of crap, anyone in medical science that categorizes those conditions as being “mild,” is simply lying. I could write an entire book filled with other examples.
But, remember, if someone has lied to you once, they can easily be lying to you again. I mean seriously, after what I’ve seen, there is simply no way I can trust almost any of it. I can only urge you to be careful and skeptical of claims by the so-called experts. Therefore, the next time you hear, or read “the study says: x,” you can confidently say to yourself “quite possibly, what the study says is complete bullshit!”
The next time you hear someone claiming (or advertising) to be an expert in chronic autoimmune disease, please call them out on it. You can confidently look them straight in the eye, and tell them that they are completely full of it. To test them, ask them why is it they cannot see that this disease is obviously a poisoning? The next time you hear someone claim that vaccines are safe and effective, you can look them straight in the face, and with complete confidence tell them they are simply either uninformed or lying. Then tell them that if they continue to be uninformed, or continue to lie, then they are complicit in the killing of children (no drama here, it’s just the facts).
The next time you hear, or read “the experts say,” you can confidently ask “says who?”, and ask “what experts?” Ask “if they are such experts, how is it that an astonishing number of people continue to be sick?”
If they are such experts why is it that we, as a society, are now 500 to 1,000 times worse off disease-wise than we were just 50 years ago? Then, ask them how many people have the so-called “experts” absolutely cured of the disease on their specialty, and cured them for life, and have done so without “side-effects?” That’s right, ask them to simply “prove it.” Whereas, real experts in all other fields of science, and technology solve real problems, have ample real-world cases demonstrating and proving their knowledge and skill. Additionally, all other fields of science have made enormous advances over the last 50 years. Whereas, regarding the chronic diseases, the real-world facts for the medical sciences show almost no progress what-so-ever. It would be one thing if they had just stagnated, and stood still regarding the chronic diseases. But, not even that’s the case; the real-world evidence clearly shows that we’ve gone backwards, and we now have disease rates far worse, and our children are plagued with mysterious new epidemics such as autism. I mean seriously, do you realize that after more than seventy years of intensive research, and sucking tens of trillions of dollars out of the worldwide economy, that the “experts” have not solved a single non-infectious chronic disease? That’s correct; not a single chronic disease has been conquered. Not diabetes, not heart disease, not stroke, not kidney disease, not arthritis, not epilepsy, not IBD, not Lupus, not eczema, not asthma, not autism, not cataracts, not Alzheimer’s, not Parkinson's, not MS, not Sjogren's, and of course, not cancer either. The same applies to government funded research. After hundreds of billions of taxpayer dollars spent, there’s no tangible results what-so-ever. How can that be possible? Well, it’s rather damn difficult to solve chronic diseases if you don’t have the faintest clue that they are, in actuality, chronic poisonings. And, yes, every single last one of the above listed chronic diseases is indeed a poisoning.
Next, ask, how many people have the medical “experts” actually killed by prescribing dubious, poisonous, and addicting drugs? Further probe their claims to being the “experts,” and ask them to prove their expertise by showing you their definitive real-world results. For many of the so-called experts in medicine, the façade will quickly crack and crumble, and their house of cards will fall apart.
Sadly, for many of the doctors in the chronic disease business, they have simply been turned into slick and sophisticated sounding front line salespeople for the pharmaceutical racket. It is a ginormous racket that now sucks trillions of dollars out of the world economy every year. Could it be that we’ve been deliberately poisoned into disease to fuel the profits of the pharmaceutical industry? I don’t know, but what I do know is that it is most certainly possible. One of the primary reasons that I believe it is most certainly possible is the patent and blatant frauds I’ve come across in just a mere few hours of my research. But, of course, this systemic fraud is not just my opinion, it turns out it’s rather well known about.
NEJM’s former editor, Marcia Angell, issued this statement in 2009, after 20 years of being in the business:
It is simply no longer possible to believe much of the clinical research that is published or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.
Naturally, with massive amounts of money being involved in this industry, it attracts widespread corruption. Here’s a statement from the WHO’s Fact Sheet No. 335:
Unethical practices in the medicines chain
The medicines chain refers to the steps required for the creation, regulation, management and consumption of pharmaceuticals. Corruption in the pharmaceutical sector occurs throughout all stages of the medicines chain, from research and development to dispensing and promotion.
…
Unethical practices along the chain can take many forms such as falsification of evidence, mismanagement of conflict of interest, or bribery.
33 Disease Maps: Epidemics on the Ground, By Tom Koch, University of Chicago Press, Jun 30, 2011 - History - 330 pages
As a I wrote about in my previous e-book, the fraud I was seeing in the Accutane Causal Association report was indeed awfully unscrupulous, and almost outrageous. However, I was quickly learning about many more pharmaceutical drugs that are killing patients at record rates. The current estimates are somewhere in the range of about 200,000 people per year in the USA alone are being killed by pharmaceutical drugs, and that is when the drugs are used as prescribed too.34 So, although knowing that Accutane and the other brand named versions of the “drug” were destroying the lives of thousands of young teenagers, and even killing some of them, it was just a standard part of the industry’s modus operandi. Yes, killing patients was just a regular part of doing business, even if it is kids. It’s nothing I should get too alarmed about. For the industry, it’s nothing personal; it’s just business. So, with that Accutane Causal Association report, it was rather obvious to me that the conclusions being made in it were to protect only the interests of the specific pharmaceutical companies selling the product. Yes, it was simply protecting the ongoing poisoning for profits racket. This then brings us to the next vitamin-A related report that I was seeing massive fraud in, and it is a doozy.
It’s a report investigating the potential cancer-causing effects of Vitamin-A Palmitate. If you’ve read my previous e-book, what you should be getting a pretty good understanding of is that vitamin-A palmitate is what should otherwise be known as the slow poisoning of the entire Western world! The vitamin-A palmitate added to our staple foods is a manmade molecule. It is manufactured by combining vitamin-A with palmitic acid (a fat). But, vitamin-A palmitate is a dirty, sneaky trick to play on the body. When cells believe that they are taking up a lipid, it’s really a toxic lipid because it now has the vitamin-A molecule attached to it. For the most part, in the context of all human evolution, this molecule is completely unnatural in the human body. Not only is vitamin-A palmitate added to our foods, but it’s also added to many cosmetic products, including many sunscreens. The primary reason it is in these products is that of the perceived growth stimulating effect it has on skin cells.
A couple of decades back, some parents in Demark started to notice that their kids who had developed skin cancers, the cancers appeared where they had applied the most amounts of sunscreens. Of course, to the medical experts, that did not make any sense, and the concerns raised by these parents appeared to be nonsense. The dismissive response was like; no, these foolish parents knew nothing about science, and cancer, and therefore they must have just been imagining this association. Nonetheless, there were some early European studies conducted to investigate a possible link, and sure enough, there did indeed appear to be a connection with the higher use of sunscreens and the probability of getting skin cancers. Under considerable pressure, the regulatory agencies in the United States then conducted their own study into the matter. It is: Photococarcinogenesis Study of Retinoic Acid and Retinyl Palmitate
 |
This report, published in 2012 has about 30 authors / contributors signed on to it. It is a one-year study that has taken over ten years to complete and release. As you read this 350-page whopper, the propaganda should become rather apparent.
Firstly, it talks up most of the known benefits of vitamin-A. Right away, that’s a bit odd to see an upfront bias in what should be an objective investigative report. Why are they talking up the benefits of vitamin-A at all, when they are supposed to be impartially investigating its potential link to it causing skin cancer?
Next, they describe the detailed mixture of the “control cream” they use in the experiments. Of course, all sunscreens have a base cream component to them. Basically, for these researchers, their thinking is that it might not be just the vitamin-A palmitate in the sunscreens that’s responsible for causing cancers, it may be some compound in its base creams. So, what they do with their experimental control cream in these experiments is juice it up with other known carcinogens that they claim is in a variety of cosmetic products.
Right away, this action introduces more variables into their experiments, and no legitimate scientists would do such a thing. Yet, based upon this illogical thinking they essentially deem their “control cream” as being their baseline “placebo.” Of course, any true “placebo” control cream would have absolutely no known carcinogenic effects to it.
Next, they put a significant emphasis throughout the report on the fact that they’ve used Simulated Sunlight – SSL in their experiments. This introduces yet another obfuscating factor into their experimental results; maybe it was the use of the SSL, and that exposure to real sunlight might not be so bad kind of thinking.
Next, they talk up the well-known fact that sunlight alone, without sunscreens, can and does indeed cause cancer - implying it’s the public's fault. Yes, they want to foist the blame on the general-public for the escalating rates of skin cancer, claiming that we are just spending too much time in the sun. However, you can disprove this theory with just two minutes of investigation, Firstly, Americans are now spending significantly less time in the sun than compared to a decade ago. Secondly, due to atmospheric pollution the intensity of sunlight striking the surface of the earth is now significantly lower too. Yet, in the face of those facts our skin cancer rates have soared over 300% in the last two decades.
Completely disregarding these facts, and ignoring millions of years of our human evolution living in the sun, it’s like they are almost trying to throw up any excuse they can think of to blur and distract from the real results. But, then the comments go beyond being irrational excuses and move into the realm of being completely absurd. One claim is that the mice scratching themselves may have caused some of their skin cancers!
Next, they talk up the use of retinoids in dermatology in helping photodamaged skin. They also talk up the “chemopreventive actions” of retinoids. They pretty much claim that vitamin-A Palmitate is a great molecule because it more readily accumulates in tissue than what regular vitamin-A does. They claim that vitamin-A Palmitate is the primary storage form in the skin - yet they skim over the little detail that it is a synthetic molecule, and therefore, it should maybe not be accumulating in the skin at all. And, even though this is America, more is not always better.
Next, the commentary goes even more completely nutty. Although the report authors correctly state that the retinoids are very highly light absorbing, they claim it this offers some protection. Implying that the molecule is acting like a little mini sun shield. But they know full well that it is exactly the opposite; it will cause the containing tissues to absorb more light energy. Of course, there’s no mention that by absorbing that larger amount of light energy, the cells containing the retinoids are going to become differentially heated, and it also provides activation energy to start decomposition chemical reactions of the retinoids. There’s no mention of that the elevated contents of retinoids will be drawing more light energy into the cell’s nucleus and causing DNA damage to them. They know all of this because they have their prior report published in 2005 detailing the processes, titled: The Photodecomposition and Phototoxicity of Natural Retinoids.
They also state that when people do have adverse reactions to treatments with retinoids, it’s usually mild and not long lasting. However, in no way do the above contradictions and statements that I’m pointing out here, along with their clear biases and lack of objectivity, constitute scientific fraud. No, that is just bad scientific practice. We need to dig just a little bit deeper to see the real fraud.
Let’s start with some of the little lies. On page 125, regarding retinoic-acid (RA) they state:
Mild-to-moderate skin reactions such as erythema, peeling, and burning are among the most common reported side effects associated with use of topical RA. Generally, the side effects subside with time and do not limit the use of topical RA.
However, this statement is not true. If you read dermatology textbooks, this common occurrence of erythema, peeling, and burning is exactly the reason treatments with RA are forced to be limited.
Then we get deeper into it. Although the usual concentrations of RA in cosmetics range from 0.025% to 0.1% (Bombei, 2009), in this study they hugely scale it back:
In the current study, the RA cream was composed of the base cream (85%), RA (0.001%), and diisopropyl adipate (15%).
Therefore, they are testing with creams that are one hundred times less concentrated in RA, and for retinol palmitate (RP) it is about ten times less concentrated than in the average found in sunscreens. Even so, the experimental results they demonstrate with RA are clearly troubling:
In male and female mice exposed to SSL, there were statistically significant decreases in survival among groups treated with RA when compared with groups treated with control cream and exposed to the same level of SSL. The decrease in survival occurred in male mice even in the absence of SSL exposure, and survival decreased to a greater extent in male and female mice exposed to the higher levels of SSL. Concomitant with decreases in survival, significant decreases in the weeks to in-life skin lesion onset were observed in male and female mice treated with the 0.001% RA cream and exposed to SSL when compared to control cream treated mice that received the same level of SSL.
and
The RA creams used in this study were not well tolerated by mice, and significant skin irritation developed in the RA-treated animals, even though the concentration of RA was well below the 0.05% used by Halliday et al. (2000) and below the lower concentration of 0.025% found in most cosmetics. Mild to severe skin erythema, peeling, sores, and scratching were noted in the clinical observations of these mice. The animal skins became cracked and ruptured, either from self-mutilation or from the application of the creams, and this resulted in 60% or more of the animals being removed from the study due to skin conditions that were inconsistent with the welfare of the animals. At a meeting of the Toxicology Study Selection and Review Committee in November 2004, a decision was made to exclude these animals from histopathology examination due to the fact that the condition of the skins of mice compromised the objectives of the study and because animals that received the 0.001% RA creams were removed at a time that was too early to develop skin neoplasms that were consistent with the development of SSL-induced skin tumors.
The same goes for retinol palmitate.
As with the RA cream treated mice, the animal skins became cracked and ruptured, either from self-mutilation or from the application of the creams, and resulted in 60% or more of the animals being removed from the study due to skin conditions that were inconsistent with the welfare of the animals. At a meeting of the Toxicology Study Selection and Review Committee in November 2004, a decision was made to exclude these animals from histopathology examination due to the fact that the condition of the skins of mice compromised the objectives of the study and because animals were removed at a time that was insufficient to develop skin lesions that were consistent with the development of SSL-induced skin tumors.
The bizarre shit just piles up higher here: Page 127
One can only speculate as to the nature of the skin irritation found in the groups of animals that received the 0.001% RA and the 1.0% and 2.0% RP creams. 1) The irritative potential of RA and other retinoids is well established, and skin irritancy may partially be explained by an overload of nonphysiological amounts of exogenous retinoids in the skin (Fluhr et al., 1999). Others, however, have used higher concentrations of RA than those used in this study and in the same mouse model without an adverse effect (Kelly et al., 1989; Kligman, 1989, 1996). 2) The mouse model may have demonstrated enhanced sensitivity to RA, RP, or to UV radiation exposure.
Let’s think about this: “One can only speculate as to the nature of the skin irritation found in the groups of animals that received the 0.001% RA and the 1.0% and 2.0% RP creams.” statement a bit.
Basically, what they are asking is, “how can such apparently low doses of the retinoids be causing these severe reactions?” Stunningly, they answer is staring them in the face. They don’t need to speculate at all. The material fact is that it is happening. Therefore, the clear answer is that even at the levels of 0.001% RA and the 1.0% and 2.0% RP, these concentrations in the creams are indeed toxic.
But, there’s no getting around it, and whether they can believe their own eyes or not, the results are conclusive that the retinoids are indeed causing higher rates of skin cancers. Here are some comments from their conclusions:
Retinoic Acid
Compared to the control cream, RA further enhanced the effects of SSL in SKH-1 mice based upon earlier onsets and increased multiplicities of in-life skin lesions.
Retinyl Palmitate
Compared to the control cream, RP further enhanced the effects of SSL in SKH-1 mice based upon earlier onsets and increased multiplicities of in-life skin lesions.
Compared to the control cream, RP further enhanced the photocarcinogenic activity of SSL in SKH-1 mice based upon increased incidences and multiplicities of squamous cell neoplasms of the skin.
 |
So, yes, there is absolutely a photo-carcinogenic effect of retinol palmitate. At right is a combined summary of what they’ve reported. Please note that the SSL treatment used in these experiments is the equivalent of only 9 minutes of Florida noon time sun daily.
Therefore, for the retinol palmitate creamed animals, they are getting cancers at a rate of 52.8%, as opposed to only 22.2% of those on the control cream. So, that’s a whopping 81.6% difference between the two groups. But, of course, we need to remember that their “control cream” has been rigged with cancer causing agents too. But, that’s not the real fraud here. Not at all. Did you spot the real fraud?
It’s this:
The RA creams used in this study were not well tolerated by mice, and significant skin irritation developed in the RA-treated animals, even though the concentration of RA was well below the 0.05% used by Halliday et al. (2000) and below the lower concentration of 0.025% found in most cosmetics. Mild to severe skin erythema, peeling, sores, and scratching were noted in the clinical observations of these mice. The animal skins became cracked and ruptured, either from self-mutilation or from the application of the creams, and this resulted in 60% or more of the animals being removed from the study due to skin conditions that were inconsistent with the welfare of the animals. At a meeting of the Toxicology Study Selection and Review Committee in November 2004, a decision was made to exclude these animals from histopathology examination due to the fact that the condition of the skins of mice compromised the objectives of the study and because animals that received the 0.001% RA creams were removed at a time that was too early to develop skin neoplasms that were consistent with the development of SSL-induced skin tumors.
The somewhat sneaky fraud going on here is that they preemptively removed 60% or more of the animals because they were showing early signs of having adverse reactions. Meaning, the more susceptible animals, the ones showing the signs of the very condition they were supposed to be looking for, were removed from the study. The same goes for the retinol palmitate group:
As with the RA cream treated mice, the animal skins became cracked and ruptured, either from self-mutilation or from the application of the creams, and resulted in 60% or more of the animals being removed from the study due to skin conditions that were inconsistent with the welfare of the animals. At a meeting of the Toxicology Study Selection and Review Committee in November 2004, a decision was made to exclude these animals from histopathology examination due to the fact that the condition of the skins of mice compromised the objectives of the study and because animals were removed at a time that was insufficient to develop skin lesions that were consistent with the development of SSL-induced skin tumors.
Next, let’s start to ask some sticky questions here. Firstly, they state their reason for removing these animals from the study was that it was: inconsistent with the welfare of the animals. Huh? Seriously, does anyone believe that nonsense? By this point in time, millions and millions of mice have been sacrificed (and often effectively tortured to death) in the name of scientific research, and suddenly these people get a conscience about it, and right in the middle of their critical cancer causation experiment too? Why did they get a conscience about what was happening to mice that they are deliberately trying to induce cancer in? Okay, so what exactly happened to the mice after they were so humanely removed from the experiment? Most likely, it was straight to the incinerator with them.
But, vastly, and hugely more important, these esteemed researchers are supposed to be investigating a serious potential cause of skin cancer in humans, and of course, many of these cases will be in kids. What legitimate scientist, after seeing that these animals are starting to display exactly the condition they are testing for, would prematurely remove the animals from the experiments? No, no legitimate scientist would do such a thing. Even if grade nine students did such a thing in a science project, they’d get a big fat ‘F’ for it. However, for these so-called researchers, I think they should get a big fat ‘F’ for Fraud.
34 https://www.youtube.com/watch?v=mqceOdDzWLQ
If the video has been removed from YouTube, click [HERE] to view a saved copy of this video in a popup window.
Moving along, some additional questions are needed to be asked here. Why do they use this vague approximation and state: “resulted in 60% or more of the animals” when the number is not an analog value? The count of mice removed is an integer value. Why state this vague 60% or more value? Why not state the exact number of animals explicitly? Was it really 65, 73, or 75 of the animals that were taken out of the study?
Another hugely important question is: what exactly was that condition occurring in these early presenters resulting in: “mild to severe skin erythema, peeling, sores, and scratching were noted in the clinical observations of these mice. The animal skins became cracked and ruptured, either from self-mutilation or from the application of the creams?”
Was that inflamed skin condition really eczema, psoriasis, or did it maybe even include the symptoms of xerophthalmia? Did any of the animals have asthma, or diabetes, etc.? I guess these investigators weren’t inquisitive enough to investigate that, nor had any interest in finding out. And they were apparently also not curious enough to find out why the animals were so profusely scratching themselves to the point of “self-mutilation?” Likewise, of all the animals that survived the early culling, and went on to develop skin cancers, how many of these also had other cancers of the internal organs? Of course, there’s not a word about investigating any of these possibilities either.
Obviously, since they removed more than 60% of the mice, who were presenting early disease conditions, we know that the real increase in the rates of induced skin cancer are much higher than what they report, and it’s more likely in the range of 80 to 90%. However, we don’t really have to speculate too much, because when we see what happens when we compare the group of animals that received no cream whatsoever (the previous numbers that are shown above where the rates jumped up from 22.2% to 52.8% were between the rigged control cream and RP groups).
Here, in the comparison between the no-cream group and the vitamin-A palmitate group, there is an even bigger jump. The numbers are shown below:
Squamous Cell Papilloma, Squamous Cell Carcinoma in situ, and/or Squamous Cell Carcinoma
No Cream @ 6.85 mJ•CIE/cm2 - 7/35 (20.0%)
0.5% RP Cream @ 6.85 mJ•CIE/cm2 - 35/35 (100.0%)
0.5% RP Cream @ 13.7 mJ•CIE/cm2 - 36/36 (100.0%)
From these numbers, the cancer rates are at least 5 times higher in the animals treated with retinol palmitate. The reason I say at least 5 times higher, is because you can’t get higher than 100% in the cancer incidence rates as seen in the two RP groups. Even more astonishing is that the numbers shown above exclude the early presenting animals prematurely culled from the study. Therefore, the true rate increase will be much higher than 5 times. Who knows what the real number is? It’s abundantly clear that these investigators are in no hurry to find out either.
Even though in the introduction to the report, they hyped up the beneficial features of vitamin-A palmitate being more readily accumulated in tissues, they fail to mention even one word about it having been added to the national dairy supply since the mid-1970s. That’s correct; there’s not one word in this study about supplemented milk, dairy, margarine, etc, and of course infant formulas too. There’s not one word about breakfast cereals, or other foods being supplemented with vitamin-A. Of course, they know full well that the vitamin-A palmitate added to sunscreens is only one source, and a much smaller one, of the overall amount of it getting into the human body and subsequently collecting in the skin lipids.
Additionally, there’s not one word mentioned that the vitamin-A palmitate in the sunscreens is the same molecule as what’s added to your kid’s milk. Of course, they know that the dietary intake via fortified dairy will also be accumulating in the skin lipids and sebaceous glands too. They know that this will be slowly poisoning people from the inside-out as much as it will be from the outside-in. Therefore, vitamin-A palmitate will be accumulating in even the skin of people who have never used a sunscreen.
So now, why do you think we have an epidemic of soft tissue cancers, including skin cancers? Do you think they did not figure this out in the ten years it took for them to write up this study? What in the hell were they really doing in those ten years?
Based upon their own report, vitamin-A palmitate supplementation might be accounting for 80% of the North American skin cancers. That’s about 3.2 million people per year, or about 32 million people over the last 10 years, while they’ve been thinking about it. On the one hand, I can see why they’d want to hush that up. But, on the other hand, are these people not charged with protecting the public health? Are they not being paid by taxpayers to be on guard, and on the lookout for exactly what they are seeing in this report?
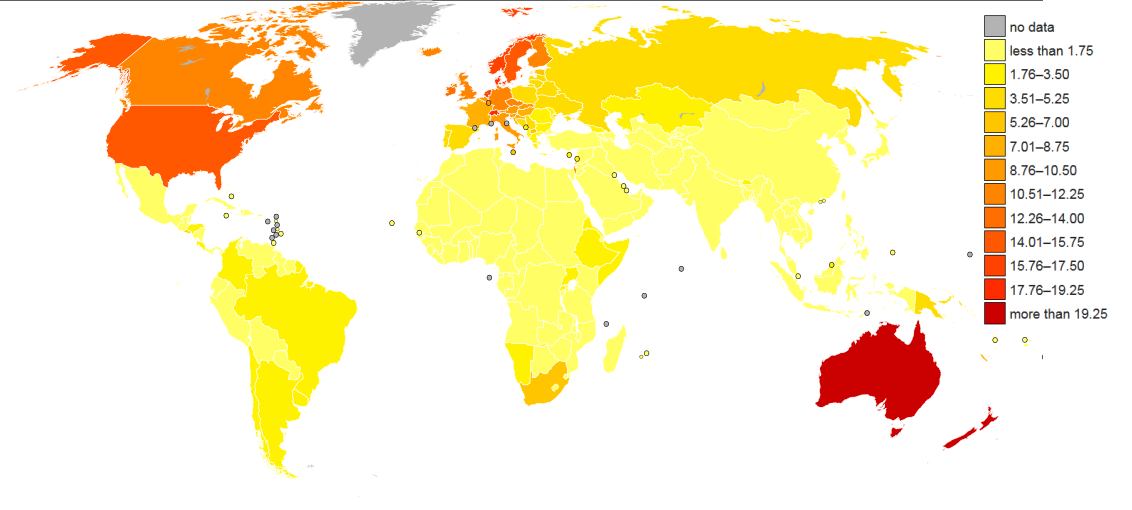
Figure 23 Worldwide Melanoma of Skin Cancer Incidence - 2008
Original Image source: https://en.wikipedia.org/wiki/File:Worldwide_Melanoma_of_Skin_Cancer_Incidence_-_2008_Globocan.svg |
As for their claim that it’s just over exposure to the sun that’s causing the epidemic rates of skin cancers we have in North America, then they need to explain this map:
If there were any merit to the claim that it’s just overexposure to sunlight responsible for causing the higher rates of skin cancers, then we should see a big bright band of significantly higher rates at the equator right around the planet. Of course, it’s just the opposite. The countries with the highest rates are the Western (and other NATO) countries that are supplementing their staple dairy products with vitamin-A palmitate. Yes, even a 9th grader can clearly see that this is a man-made problem.
Yet, they try to obfuscate this glaring reality and try to pin the blame on the excess light having caused the cancers in their experimental animals.
Here are their stated conclusions:
The RP Study Results and Conclusions
As expected, exposure to synthetic solar light resulted in a variety of skin cancers in the mice. Mice given the carrier creams in addition to light exposure developed more tumors per animal, with a shorter time before the appearance of tumors. Mice given creams containing retinyl palmitate or retinoic acid had even more tumors and earlier onset of tumors than animals given the carrier cream, both with and without exposure to the synthetic solar light.
and
Conclusions
We conclude that treatment with the carrier cream increased the incidence of skin tumors in hairless mice, both in the presence and absence of synthetic solar light. Inclusion of retinoic acid or retinyl palmitate in the cream increased the number of tumors and decreased the time to appearance of tumors compared to animals given just the carrier cream.
Thus, after ten years of deep thought, and analysis they conclude: it’s the carrier creams. Yes, they are hoping we are so gullible to buy this “it’s the carrier creams” bullshit. Just as amazingly, after ten years, and who knows how much taxpayer money spent on this report, their conclusion is given in just two sentences. They further try to somewhat conceal the real truth – by claiming it is the inclusion of the retinol palmitate in the nasty carrier cream (the one they’ve juiced up with carcinogens), and not the retinol palmitate alone to blame.
Okay, let’s move along to the next aspect of this report. We’ve all been led to believe that the peer-reviewed papers are the “gold standard” in medical research. So, let’s see what happens with the peer-review process on this study.
SUMMARY OF PEER REVIEW PANEL COMMENTS Page 15.
Dr. M.E. Ginevan, an independent consultant hired by PCPC to analyze the study and its results, said the group was pleased by the well-defined charge to the NTP panel. He noted the interval between the nomination and the report (11 years) and questioned the reasons listed for removing animals from the study, suggesting they may have skewed the results, leading to incorrect statistical analysis of outcomes. He said the effects of RP independent from those of the control cream could not be estimated, and the control cream itself was “a potent carcinogen” and that this was an “inadequate study of carcinogenic activity.”
Dr. M.E. Ginevan, of course, has spotted the same issues that I have with the report. However, he’s being more politically correct, and states: “questioned the reasons listed for removing animals from the study, suggesting they may have skewed the results, leading to an incorrect statistical analysis of outcomes.”
Of course, seeing the preemptive removal of more than 60% of the animals and claiming that it has skewed the results, is a colossal understatement.
And then here’s how the report authors address these concerns from their peer-reviewer:
Dr. Rice’s - first primary reviewer
Dr. M.E. Ginevan, an independent consultant hired by PCPC to analyze the study and its results, said the group was pleased by the well-defined charge to the NTP panel. He noted the interval between the nomination and the report (11 years) and questioned the reasons listed for removing animals from the study, suggesting they may have skewed the results, leading to incorrect statistical analysis of outcomes. He said the effects of RP independent from those of the control cream could not be estimated, and the control cream itself was “a potent carcinogen” and that this was an “inadequate study of carcinogenic activity.”
Basically, they just repeat Dr. Ginevan’s concerns and move on with it. There’s nothing to see here, nothing to be concerned about. In a nutshell, the wonderful peer review process is just swept aside and rendered completely meaningless.
For me, this report is a bunch of distracting rubbish, and a complete waste of taxpayer’s money. Now, here’s my conclusion and armchair review of this report:
- It’s blatant scientific fraud.
- Even with them trying to cover it up, it still points to a hugely increased rates of skin cancer being caused by vitamin-A-palmitate, it may be as high as ~ 80%.
- They rig their “control” cream by spiking it up with proven carcinogens.
- They blame 1) Sunlight 2) The control cream 3) RP only when it’s added to the control cream.
- They claim that some of the cancers are due to mice scratching themselves (ha, that’s a good one guys).
- They test with 1/100th the normal concentration of RA, and 1/10th the normal concentration of RP.
- They use only 9 minutes of Simulated Sunlight per day - SSL - why not test with real sunlight, and for much longer?
- They remove over 60% of the early presenters - due to “animal welfare concerns” - hugely skewing the resulting data.
- There are other attempts at disguising the real results.
- They gloss over the colossal importance of their indisputable findings.
- They don’t consider or look for other internal cancers they may have induced.
- They don’t investigate what the non-cancerous lesions are that they have induced either? For example, were these animals presenting with eczema?
Where are all the great dermatologists on this nonsense report? Silent, of course. Where are all the other great cancer researchers on this report? Silent, of course. It’s almost complete silence all-around on this study and report. Why?
Even based on the numbers presented in this report, vitamin-A palmitate (from supplemented foods, and sunscreens combined) is most likely responsible for at least 3.2 million new cases of skin cancer each year. Therefore, for people to remain silent on this report’s finding is criminal negligence at best.
So, why are the authors on this report not sounding the alarm? Surely, they were seeing the results, and they knew exactly what they were looking at. There can be no doubt about that. Unlike the Accutane study, there’s not just a few manufacturers to be protected here. So, why are they so deliberately and desperately trying to protect a molecule? Could it be that they’ve decided to protect the ongoing profits of the skin cancer industry that’s raking in over eight billion dollars per year in the USA alone? Regardless of their motivations, their conduct in this report goes way beyond simply being criminal negligence causing massive amounts of bodily harm and death. When you realize that there are now about 4.5 million Americans a year being diagnosed with skin cancer, and every hour another American dies from it, the significance becomes clear. On a worldwide scale the numbers are gigantic, and of course many of the victims are children. Therefore, the cover-up and fraud they’ve committed in this report probably qualifies as being a crime against humanity. With that, they should all be sent to a Florida prison for the rest of their lives. But, that’s not good enough. They then need to have all their meals supplemented with that “safe and effective” vitamin-A palmitate, and each of them get exposed to nine minutes of noon-time sun daily. When their skin breaks out into blistering, burning, pre-cancerous lesions we’ll tell them just not to scratch themselves, as that scratching might lead to cancer. I could go on, but I think you get the idea.
However, what I do know is that this study must be repeated. It must be repeated by groups of parents, and not these biased, compromised so-called researchers. The medical establishment has no magic monopoly on who does experiments, and clearly, we can’t trust these people with some vested interest in the outcome of this crucially important work.
The experiment needs to be repeated with real sunscreens, and real sunlight too. It can be done in less than a year. The results can be made available within weeks of it being completed. Not only do we need the real numbers for the rate increases in skin cancers due to the use of retinol palmitate, but we also need to get the numbers for the rate increases for other internal cancers too. Likewise, we need the real numbers for the rate increases in non-cancerous skin lesions. Very importantly, we need the numbers of how many animals succumb to their retinol-palmitate-induced cancers and die from it. Therefore, I’d love to see a one-year cancer study comparing two groups of mice; one group on a zero vitamin-A diet, and the other on retinol palmitate, with it being delivered from both the inside and out. And with both groups of animals getting exposed to exactly the same amounts of real sunlight. Let’s see how wonderful their retinol palmitate truly is.
Next up, vaccine fraud, and it’s a doozy too.
You are probably aware of the big plastics scare a that happened a few years back, with a chemical named bisphenol A (PBA). It was uncovered that many consumer hard plastics used in food containers, including water and baby bottles, contained PBAs. The problem is that bisphenol is known to be rather toxic, possibly causing cancer and other serious health issues. Therefore, the fear was that some of it could leach out of the plastic and into the food kept in the container. To the plastics and chemical engineers, this fear was considered rather unfounded because the bisphenol molecule was tightly coupled with polymers, and if any of it was going to leach out into the food, it was scant little to none, and it was not going to be in a free form. Therefore, in their view, the chance of it being a serious risk to health was exceedingly small. However, to the alarmed consumer advocates, they were having none of that argument, and millions of kilos of perfectly good plastics were sent to our landfills.
Of course, to many parents, the thinking was regardless of how minuscule the risk, they were just not going to take any chances when it comes to their children’s health. To the general consumer, they were going to err on the side of caution too. Thinking, let’s not take any chances with cancer. The FDA has ended its approval of the use of BPA in baby bottles (due to market realities, rather than safety). But, Canada and the European Union has banned the use of BPAs in baby bottles due to safety concerns.
Therefore, today, when you go out to buy a nice hard plastic water bottle almost all the products available proudly display a BPA-Free logo, or banner. Okay, fair enough. In my view, it was all a big over reaction. I was on the side of the chemists and plastics engineers; I felt that the real risk was indeed relatively darn small. Nonetheless, here we are today. So, what is it that makes the bisphenol molecule so toxic? Well, bisphenol is really two much simpler phenol molecules bound together, and phenol is extremely toxic.
Phenol Toxicity: “Its corrosive effect on skin and mucous membranes is due to a protein-degenerating effect. Repeated or prolonged skin contact with phenol may cause dermatitis, or even second and third-degree burns. Inhalation of phenol vapor may cause lung edema. The substance may cause harmful effects on the central nervous system and heart, resulting in dysrhythmia, seizures, and coma.
So, this tiny, simple molecule, is shockingly damn nasty. The reason it is so toxic is because of the hydrophobic (fat-soluble) benzene ring and the attached OH group making it a highly reactive acid that rapidly destroys proteins and slips its way into cells. Phenol goes by other names; including carbolic acid, benzenol, phenylic acid, hydroxybenzene, and phenic acid. Phenol is a very well-known molecule in chemistry. The basic mechanism of it toxicity is that it quickly substitutes itself into the similar cyclohexane ring structures on the RNA molecule. Its toxicity is amazingly fast acting, and its devastating effects on the skin and other tissues have been well known since at least the 1930s. Just how fast acting is it? At high doses, it can cause death within just 15 seconds.

Of course, we wouldn’t expect the Nazi’s not to have taken notice of this fast-acting chemical killer. And, oh yes, they sure did. Before the Nazi’s doctors had their death-camp gas chambers and ovens working on a full tilt industrial scale, they were killing their prisoners by injecting them with phenol. It was a simple phenol in an aqueous solution (in water) injected via medical syringe. In the early days, they were injecting it into a vein, and then a bit later as they refined the technique, directly into the heart. When injected into the heart, it usually killed an adult within 10 to 15 seconds. Of course, phenol was used to execute countless children too in these death camps.
Somewhat bizarrely, following official protocol, to administer an injection it was deemed to needed to be done by doctors. Therefore, what should have been medical healers were now assembly line serial killers using a “medical” procedure. Very oddly, some of the doctors were even pre-wiping the injection site with alcohol swabs, you know, just to keep the site sterile and follow the official medical ceremony for doing injections.
Figure 24 Doctors killing with Syringes: Phenol Injections
|
It is estimated that the Nazi doctors killed over a 100,000 people via phenol injection. One of the most notorious of the phenol injecting doctors was the infamous Dr. Josef Mengele. The account of the phenol killings is very well detailed in Robert Lifton’s book titled: The NAZI Doctors, Medical Killing and the Psychology of Genocide.
Therefore, with that bit of history, and out of respect, I don’t care how minuscule the chances are of it causing harm, we probably just should not be including phenol in consumer products that come into regular contact with foods.
Okay, so, where’s the connection here with vaccines? Surely, no vaccine manufacturer would be including phenol, a Nazi execution drug, directly in our “Safe and Effective” vaccines? But, oh yes they are, and it is exactly the same phenol molecule too. It’s in a nice simple aqueous solution to boot, not bound to some plastic resin. So, don’t worry about some trace amount of bisphenol leaching out of your baby’s plastic bottle. The vaccine’s manufacturer has got your back on this one, it’s unbound phenol, in liquid, injected directly into the bloodstream. I mean, what could possibly go wrong with that?
Here are a few snippets directly from Merck’s product insert for their Pneumovax-23 vaccine.

Why are they injecting our nation’s infants and kids, and seniors with phenol? The lethal injectable murder weapon preferred and perfected by Nazi death camp doctors, used to murder 100,000s of victims? Have these people at Pharma companies gone completely mad? Nope; it’s awfully damn clear they simply don’t care, and just as clearly, it’s all about profits.
Even more importantly, where the hell is the CDC, the FDA, and Health Canada on this? I don’t think they care either. But, my bet is that the Jewish community might care a whole lot, and find this all rather repulsive.
Of course, someone will claim that just a little bit of aqueous phenol might not be so bad. But, that’s not what the MSD sheet35 for phenol tells us. It details exposure results such as:
- Toxic in contact with skin
- Causes severe skin burns and eye damage.
- Fatal if inhaled
- Suspected of causing genetic defects
- May cause damage to organs
- May cause damage to organs through prolonged or repeated exposure
- Much more…..
- And if a person encounters aqueous Phenol they are to Immediately call a POISON CENTER or doctor/ physician
Astonishingly, here in the vaccines the doctors and physicians are directly injecting aqueous Phenol into kids and adults! If you think that’s not bad enough, then please keep reading. Depending on just how careful the nurse is with that Pneumovax vaccine injection and if it’s not a perfect intermuscular injection, and the phenol enters directly into a blood vessel, it could then easily end up in the heart valve, brain, or some other critical tissue.
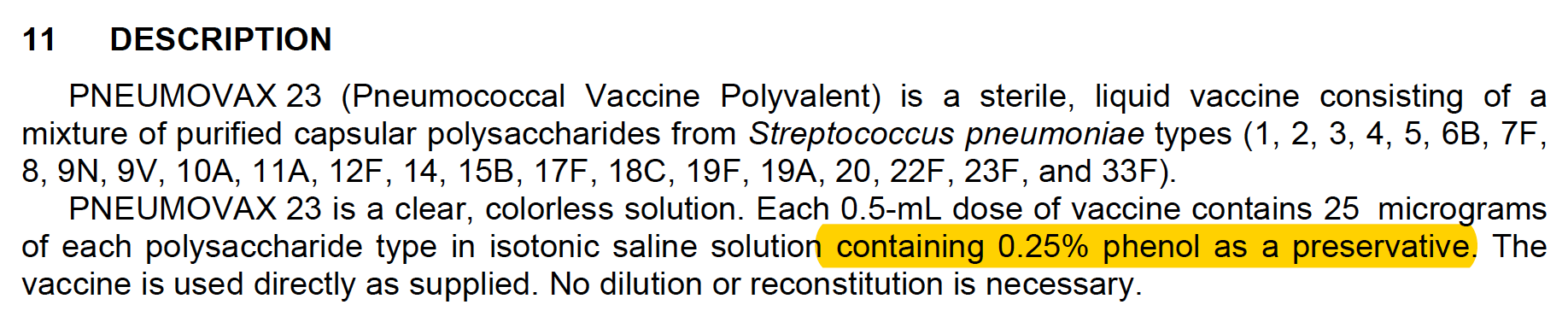
So, why in the hell would they include phenol in the vaccine in the first place? Very oddly, they have labeled it as a “preservative.” Except, phenol is not a legitimate preservative - no way, not a chance of it. That “preservative” label is a lie. Please show me any food product on the market that uses phenol as a “preservative,” and I’ll show you a lot of dead customers. That’s not just speculation either, because in the 1930s the German army ran a short-term experiment testing phenol as a food preservative. The result of that experiment was a bunch of dead soldiers. Then, later in the war years the lethality of phenol was further researched and well proven by the Nazi doctors.
The “concentrated aqueous solution of phenol” that was developed proved “inexpensive, easy-to-use, and absolutely effective when introduced into the heart ventricle.” So that an injection of 10 to 15 milliliters into the heart caused death within 15 seconds.
Source: The NAZI Doctors, page 258
Now, what is phenol really doing in the Pneumovax vaccine? Of course, it’s one of the vaccine’s adjuvants. It is a cytotoxin used to damage and kill cells, preferably near the site of injection. Without the adjuvant’s action, the vaccine has almost no chance of “working.”
If you are thinking this just can’t get any worse, think again. Yes, it gets a whole lot worse, and real fast. That’s because Phenol is in their “placebo” too! That’s right, they have rigged their “placebo” with phenol too. What a sneaky, disgustingly dirty fraud.
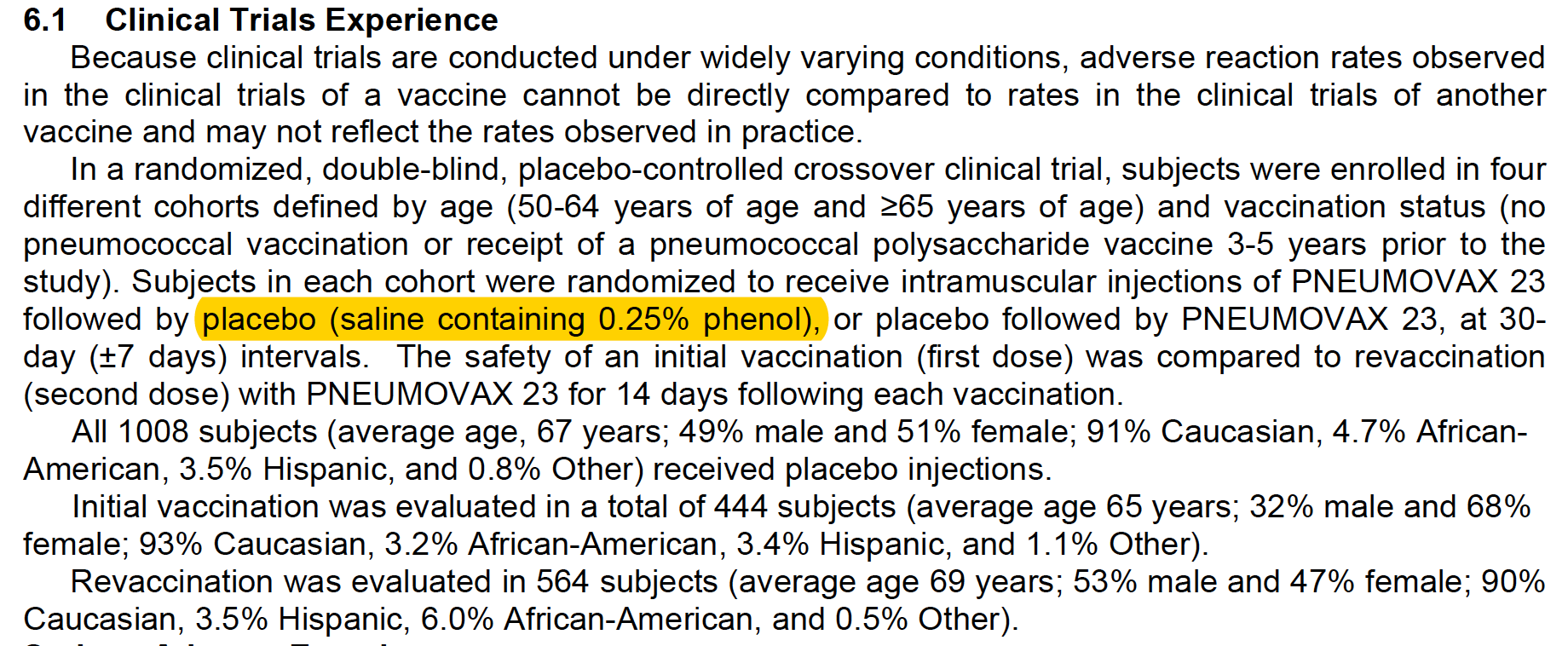
Clearly, this rigging of their placebo evens out the score on “adverse reactions,” and they get to claim that the number of adverse reactions to the vaccine is not much worse than that of the “placebo.”
Except, that’s one hell of a placebo. How can a real saline “placebo” cause heart failure, diabetes, and death? The answer is that it can’t. Moreover, why is heart failure termed just a “complication” of myocardial infarction? However, the super important and critical point I want to make about the rigged placebo study is that it proves, by their very own testing, that the concentration of phenol, at 0.25%, used in their production vaccine is at or beyond the lethal dose for some adults. Children will, of course, be much more vulnerable. Therefore, they know, and they know with absolute certainty, that the distribution of their rigged placebo tested production vaccine will be randomly killing people. And they knew that in advance of the production release too. Naturally, there should be no doubt that it continues to do so today. Therefore, this particular vaccine isn’t just poisoning for profit; it’s killing for profit. What I guess is that, for the manufacturer, it’s just another day at the office since they feel that they are protected from any repercussions.
Once again, where the hell is the FDA’s and Health Canada’s oversight on this? How can any legitimate agency scientist not see that they’ve rigged their “placebo” with a powerful, and very often lethal, cytotoxin? You really need to read Robert Jay Lifton’s book to get an appreciation of just how horrifically disgusting this phenol injection is. Some of the Nazi doctors using phenol injections to murder their prisoners were put on trial after the war, and a few were given the death penalty for doing it. Therefore, today, how can any legitimate agency scientist allow the exact same execution drug to be injected into our children? How can any pediatrician be so credulous to follow in the footsteps of Dr. Josef Mengele and inject aqueous phenol into children? How can they not have a major problem with that? Maybe, they simply don’t dare…? Of course, we need to also ask if the manufacturer has rigged this vaccine’s “placebo” testing, how many others have they rigged too?
Therefore, for me at least, this is a basic matter of trust. Seeing this flagrant scientific fraud, that is clearly going to cause deaths, how could anyone possibly trust anything these people tell us? Seriously, how can anyone trust a company that includes a known execution drug, and at a known lethal dose, in their vaccine? How could anyone trust the government regulatory agencies that have approved this vaccine? Tragically, this vaccine will be causing deaths, and severe injury, in children far more often than in adults.
Moreover, this is not the only vaccine that’s been spiked up with this horrible execution drug. The others are the Hib (PedvaxHIB), Hib/Hep B (Comvax), Smallpox(Vaccinia—ACAM2000), and the Typhoid (inactivated—Typhim Vi). In Canada, the vaccines containing phenol are: ADACEL (Tdap), ADACEL®-POLIOm (Tdap-IPV), AVAXIM (HA), ENGERIX-B (HB), IMOVAX Polio (IPV), PEDIACEL (DTaP-IPV-Hib), PNEUMOVAX 23 (Pneu-P-23), QUADRACEL (DTaP-IPV), Td ADSORBED (Td), Td POLIO ADSORBED (Td-IPV), and TYPHIM Vi (Typh-I).36
35 http://www.chemblink.com/MSDS/MSDSFiles/108-95-2_Sigma-Aldrich.pdf
Now, with knowing that the Hib (PedvaxHIB), and some other infant vaccines also contains this same execution drug, what are the chances that it is also a major causation factor in causing SIDS? To investigate this possibility, firstly, we need to know what’s the most common age for SIDS to occur at.
Although SIDS is rare, it is one of the most common causes of death in babies between 1 and 12 months of age. Most babies who die of SIDS are between the ages of 2 and 4 months.
Source: https://www.webmd.com/parenting/baby/tc/sudden-infant-death-syndrome-sids-overview
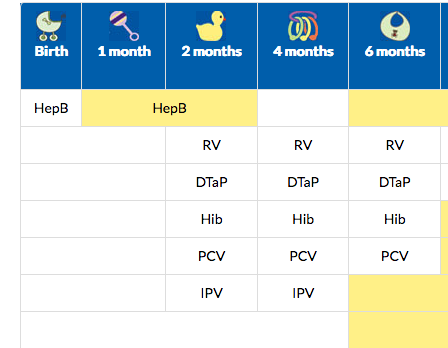
Figure 25 Snippet of the CDC’s infant vaccine schedule
Source: https://www.cdc.gov/vaccines/parents/downloads/parent-ver-sch-0-6yrs.pdf |
Next, we need to know what’s on the vaccine schedule for this same 2 to 4 months of age range. Figure 25 is a snippet from the CDC’s vaccine schedule.
Would you look at that, it’s the Hib, among others. Naturally, many of the “experts” will claim that injecting infants with a proven execution drug, and seeing them suddenly die shortly thereafter is just a coincidence. But, that coincidence claim is just about as idiotic as is the entire notion of SIDS itself. Otherwise healthy infants do not just suddenly die without some extremely powerful underlying force causing it to happen. Although that’s completely obvious, and even though medical science doesn’t know what’s causing SIDS, doctors resort to making oxymoronic rationalizations to explain it.
Although SIDS is rare, it is one of the most common causes of death in babies between 1 and 12 months of age. …
SIDS is named the cause of death only when no other cause is found.
Source: As Above
However, SIDS is not a noun, it is not a thing, and there is no “it” because SIDS is just a label applied when there is no known cause of death. Empty labels can’t kill infants, but poisonings sure can. Even more astonishing than seeing the bulk of SIDS deaths occurring in the same timeframe as when the bulk of infant vaccines are given, is that many of these mysterious SIDS deaths are occurring on the very same day as their vaccinations. Yet, almost all doctors cowardly hide behind the claim that it wasn’t the vaccines and evasively claim “it” was SIDS. That’s correct, once again rather than believing their own eyes, they’ll disgracefully claim it was SIDS (aka nothing) that killed these infants. But, since “nothing” can’t be the cause of death, why is it not then just stunningly clear to these doctors that SIDS simply must be a fatal poisoning? My guess is that the autopsies are conveniently not looking for phenol, nor measuring retinoic acid levels.
Maybe other vaccines are mostly safe for many. But, we simply don’t know exactly who they are safe on because they don’t want us to find out. If vaccines were so “safe and effective” then why does the pro-vaccine camp need to resort to committing these massive scientific frauds, and using lies, and fear mongering propaganda to promote their products? Of course, it’s because the real authority on science (nature itself) is showing us that their vaccines are causing disease, and quite often even killing our children too! They know exactly what the real science demonstrates. Clearly then, we can’t believe a single word these companies, or the medical establishment, tell us. I think we’ve had enough with the frauds and lies, and effectively the execution of our infants.
Obviously, if something were to seriously go wrong with a vaccine, let’s say a botched batch were to become contaminated with a strange foreign virus, the vaccine companies, and the medical establishment, and the government agencies would never mention a word of it to the public. They would do the exact opposite, and do everything in their power to cover it up and conceal it.
Finally, if you are still wondering why the medical research community is not getting the obvious connections here with vitamin-A and the chronic diseases, I’ll spell it out for you. Some of them are indeed getting it. Other researchers and doctors that do see it are then being told not to get it. It’s spelled: corruption.37 38
And outside of the medical research community we have the vast majority of front-line doctors who are simply in the business of perpetually treating disease, and they would never even dream about finding the root cause of a disease. But of course, there’s more to it. We need to find the answer to this question; why are they protecting the vitamin-A molecule? By 1937, and most certainly much more so by 1945 and 1947 it was abundantly clear to medical researchers that vitamin-A was incredibly toxic, and at the very least it would be causing an accelerated osteoporosis in seniors. They also knew, and they knew full well, that with it being a fat-soluble molecule it would slowly accumulate. Therefore, they knew it was just a matter of time before a large percentage of the older population moved in to a potentially toxic state with it. Some researchers in the 1940s even recommended that government make it a controlled substance. Therefore, it makes absolutely no sense whatsoever to have legislated vitamin-A into our food supply. Coincidentally, by 1960 vitamin-A was also starting to be used as a chemotherapy drug, and was thought to have some “chemo preventive” aspects to it. At least, that’s what the nice drug companies were promoting it as.
Given this background knowledge, something astonishing happens in 1970. Within the first few days of Richard Nixon taking office as the new elected 37th President of the United States, he declares his famous War on Cancer. He almost immediately allocates a hundred million dollars in research funds towards it.
1971 State of the Union address: "I will also ask for an appropriation of an extra $100 million to launch an intensive campaign to find a cure for cancer…
Source: Richard Nixon, President of the United States
But, the total spend jumps up to 2.6 billion dollars within just two years. Additionally, in around 1972, the United States Government legislates the addition of vitamin-A to all low-fat dairy. The addition of vitamin-A to the low-fat dairy is not optional for suppliers, it’s mandatory. This is a rather peculiar move, because as far as I could determine, there was absolutely no signs of widespread or endemic vitamin-A deficiency going on in the United States in this era. Of course, the excuse provided to the public was that with the removal of the milk’s fat, much of its vitamin A content had been removed too. Therefore, the vitamin-A needed to be added back. However, it’s not just vitamin A added back to the low-fat dairy, it’s also vitamin-D too. Of course, they know that vitamin-D will somewhat blunt the osteoporosis causing effects of the added vitamin-A. So, even though vitamin-D is a well-known toxin, and it’s even used as a rat poison, it’s included in the mix. Therefore, with milk containing calcium, and the government starts hugely promoting the consumer uptake of milk, they think that they have their bases covered in combating the osteoporosis that the additional supplementation of vitamin-A will be causing. Okay, so all of that seems like a pretty strange thing to legislate into the nation’s dairy supply. Was the big low-fat dairy promotion just a very sneaky and deceptive way of getting consumers to consume more vitamin-A that government thought we suddenly needed? I think that is likely. But why and where is the connection? What could have been their real motivations for them doing this? Well, I think the clue is in that thought to be “chemo preventive” aspect of vitamin A.
Was there some disastrous secret event that had taken place in the early 1960s that was so horrible, and so widespread, that the government feared there was going to be a dramatic, and wide ranging, increase in the rates of cancer? Of course, this dramatic epidemic increase in the cancer rates since around the mid 1960s has indeed happened. Right away, I suspected that there was a very large scale industrial accident that had released a cancer-causing agent into the environment. This had to be a massive release of something incredibly carcinogenic. It also had to be something that had been released in around 1962 to 1965. It also had to have been something that had been released by some of the other NATO countries at the same time too, such as Canada and the UK. The same thing had to also have happened in Australia. Of course, the NATO alliance is not just a military alliance; most of its countries also have reciprocal trade alliances too. Meaning, from an industrial-standards setting point of view, or from a food standards point of view, many of these countries try to synchronize their supplementation programs to put each nation on a level playing field so to speak. For example:
This report is one in a series that presents a comprehensive set of reference values for nutrient intakes for healthy U.S. and Canadian populations. It is a product of the Food and Nutrition Board of the Institute of Medicine (IOM) working in cooperation with Canadian scientists.
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine. National Academy of Sciences.
ISBN 0-309-07279-4
My first thought on the matter was that there was a possible wide-scale adoption of a new pesticide such as DDT, or even a massive leak of radioactive particles, say as part of some new botched high potassium content farm fertilizer. Maybe, by some weird and unforeseen set of circumstances, some radioactive isotope had been included in our foods. But, of course, just a few minutes of thinking rules out that latter possibility. There are just way too many average citizens out there with Geiger counters, and they would’ve detected such a leak.
37 https://www.youtube.com/watch?v=mqceOdDzWLQ
If the video has been removed from YouTube, click [HERE] to view a saved copy of this video in a popup window.
38 https://www.youtube.com/watch?v=s-8ItXRMPfA
If the video has been removed from YouTube, click [HERE] to view a saved copy of this video in a popup window.
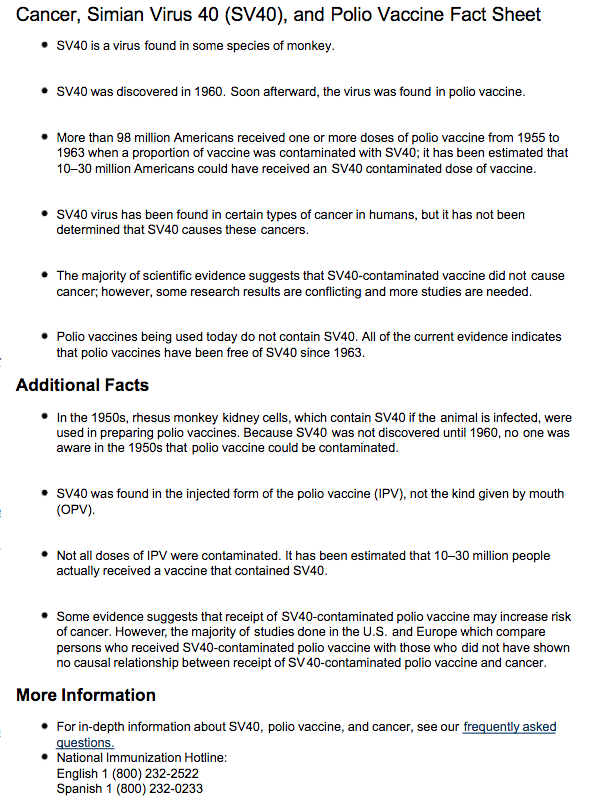
Cancer, Simian Virus (SV40), and Polio Vaccine Fact Sheet
|
Okay, so what other major event happened in around 1963, and it happened on a very wide scale, so much so that it reached beyond the United States borders into the other NATO countries? What could’ve possibly caused the massive distribution of a serious carcinogen? Well you don’t have to look very far. The prime suspect is the botched polio vaccine of 1962, and 1963. Unbeknownst to the early scientists working with, and distributing, this vaccine it was contaminated with a virus from the African green monkey. The polio viruses used in the vaccine were grown on ground-up monkey kidneys. Those monkey kidneys contained the then hidden monkey virus, and it had cross contaminated back into the vaccine batches. It is a very tiny virus that was simply not detectable with their early microscopes. However, once found, the virus was given the designation SV40 (Simian Virus # 40). Its structure is nearly identical to that of another sinister virus, one that has a more common name; it’s called the HIV virus. Therefore, some people believe that this is indeed the same virus and origin that introduced AIDS into the human population. But by the time the vaccine’s manufacturer had detected the SV40 virus contaminating their vaccine doses, it was too late. Much of it had already been distributed and administered to unsuspecting Americans. However, in the early 1960s, they had no idea what they were really looking at regarding the disease that the virus was causing. A facsimile of the “Fact Sheet” on the matter posted on the CDC’s website back in 2013 is shown above right:
Of course, back in the early 1960s they had never seen AIDS before, so to them, it appeared to be another form of cancer. And of course, AIDS often does cause real cancers too. Their initial testing on this newly discovered SV40 virus told them it was one of the fastest acting cancer causing agents they had ever seen.
We can get the account of how this fiasco came about, straight from the horse’s mouth on it, so to speak, that of Dr. Maurice Hilleman. Dr. Hilleman was one of the most prominent, and distinguished, early vaccine pioneers, and especially so for the polio vaccine developed at Merck. He describes how the foreign green monkey virus was inadvertently introduced into the live virus version of the polio vaccine. Dr. Maurice Hilleman makes some rather astounding revelations in this interview.
Naturally, the only thing governments wanted the public to know about their vaccines, and for us to continue to believe, is that – “vaccines are safe and effective.” Just remember that it’s us, the “experts” in medical science, that say so. Therefore, there was no way in hell they were going to tell the public that they had just mass inoculated all the nation’s children with what was believed to be a cancer-causing virus.
Although there was a secret program conducted looking for a magic antiviral antidote, and even other vaccine solutions, to the SV40 virus, none was found. Much of that secret research was conducted at the US Army’s Fort Detrick research facility in Maryland. This was also the research facility that received the bulk of Nixon’s cancer research funding budget.
As part of this national effort, in October 1971, the Army's Fort Detrick, Maryland, biological warfare facility was converted to a cancer research center, eventually becoming the Frederick Cancer Research and Development Center, an internationally recognized center for cancer and AIDS research.
That research effort was their plan “B” counter attack to the threat posed by the SV40 virus. But, in case that didn’t pan out, they’d already moved ahead with Plan “A.” Plan A, was to slowly dose up the entire North American population on what was thought to be the only {tip content="the prevention of disease by the use of food supplements, drugs etc."}chemo preventative{/tip} drug in existence at the time. However, I believe Plan A, using vitamin-A, was just their interim plan. It was just to buy time because surely with all the great minds working on the AIDS / Cancer research they would crack the real problem. As we now know, that did not happen.
Of course, this contaminated polio vaccine had been shipped out to other countries, including Canada and the NATO countries of Western Europe, and to Australia too. Therefore, I believe this is the real reason that vitamin-A was so aggressively added to the nations low-fat dairy supply. And this is the real reason the governments hugely funded the marketing campaigns by the dairy industry to get us to consume a lot more low-fat dairy in the 1970s and ’80s. It has been a gigantic cover-up ever since.
That is why I believe they are still protecting the vitamin-A molecule to this very day. Moreover, based on the evidence I’ve seen, vitamin A does not actually have a chemo preventative aspect to it, not at all. That claim is either based on more fake science or more big fat lies promoted by the drug companies. Thus, I believe the on-going vitamin-A deficiency theory is a big pile of lies the needs to be maintained to cover up the even bigger pile of lies then needed after they sent out the contaminated polio vaccine. Oh, what a tangled web we weave when we set out to deceive.
But, Richard Nixon did not escape this grand debacle unscathed. Rather, I believe he was a victim of it too. I suspect, given the insider information he had regarding the matter, he doubled down on his own personal dose of vitamin-A to self-medicate himself with its special thought-to-be cancer preventative qualities. Not surprisingly, it backfired on him.
By his second term, he had become completely socially incapacitated; so much so, it was impossible for him to even meet with anyone he did not already know.
Ah, uh, hmm, ah, ahh,” the president mumbled, clearing his throat and gesturing toward Haldeman. “Urm, urm.” His right hand went up to his mouth, covering it briefly. He seemed about to speak, glanced at Butterfield and motioned to Haldeman. But still there were no words. Nixon began to make little circles with his hand as if to recall something to mind. “Urm, urm,” he said. Butterfield looked pleadingly at Haldeman. Nixon again uttered some low-pitched guttural sounds that were not words. Suddenly he began to move one foot back and forth, almost pawing the carpet. It was torture. Butterfield was considering a prayer asking for divine intervention, someone to help the president, anything.
Source: THE LAST of the PRESIDENT’S MEN, By Bob Woodward.
You really should read Woodward’s book to get a better understanding of the severity of Nixon’s condition. This was no minor social phobia. Nixon was so overcome with extreme anxiety that it was impossible for him to even meet new people. Nearly every evening president Nixon ate his dinner alone too. The White House staff were protective of the president, covered for him and quite effectively kept this information away from the public.
Now, how does this dramatic mental transformation happen to a man who just a few years earlier had a huge ego, and who had an overwhelmingly type-A personality for most of his adult life too? And, of course he just happens to be the President of the United States as well. Even Nixon himself, confiding in friends, had stated that his personality had been mysteriously changed. And, very prophetically, after Watergate, Nixon is recorded to have stated : “It’s not the crime that gets you… it’s the cover up.” Tragically, the gigantic cover up is now slowly destroying our nations.
There’s much more you can learn on this topic of the contaminated polio vaccine from the great research done by Edward T. Haslam, in his in-depth investigative book titled: Dr. Mary’s Monkey.
Dr. Mary's Monkey: How the Unsolved Murder of a Doctor, a Secret Laboratory in New Orleans and Cancer-Causing Monkey Viruses are Linked to Lee Harvey Oswald, the JFK Assassination and Emerging Global Epidemics
And, no this is not some grand conspiracy theory by Haslam. It is as real-world as it gets. As shown above, for a brief time the CDC did publish some data on this event and confirmed that about 98 million Americans had been potentially exposed to a SV40 contaminated vaccine dose. Additionally, the real-world findings of the SV40 virus had been detected in human tumors by researchers in both the USA and from other countries too. Here’s just one such report (glossing over the apparent controversy issue).
Abstract
BACKGROUND:
Presently there are over 61 reports from 49 different laboratories that have detected SV40 in human mesothelioma, lymphoma, brain and bone tumors, versus three reports (two from Dr. Shah's laboratory who performed his study under contract from Dr. Strickler at the Viral Epidemiology Branch (VEB) National Cancer Institute (USA) that have failed to detect SV40 in some of these same tumor types.
https://www.ncbi.nlm.nih.gov/pubmed/12552945
Thus, based on this information and on Haslam's 20-year investigation into this disaster, the premiere and showcase vaccine supposed success story, that of eradicating polio, is probably responsible for killing at least 30 million people and doing so with the actual creation of one of the most horrible diseases imaginable. Yes, in addition to those “safe and effective” vaccines killing about 2,000 American kids each year, and inducing a massive amount of new “autoimmune” diseases, they are very likely now responsible for killing more Americans than who were killed in the last two world wars combined. However, that’s not at all the end of the story. The story is still being played out today in our extraordinary rates of the chronic diseases. Ironically, it’s not directly due to the SV40 virus, rather it’s due to the consequences of the ongoing cover-up.
Haslam describes the US government’s response to the SV40 detected in the botched polio vaccines as being the biomedical equivalent of the Manhattan Project. In the mid 1960s a massive top-secret scientific research effort was conducted looking for an anti-viral or other solution. In Haslam’s book he states that no solution was found, and the project was silently ended in failure. However, I think there’s some good evidence to indicate that what really happened is that they decided to dose up the entire nation with the only thought-to-be pre-emptive chemotherapy drug in existence. However, dosing up the entire nation on vitamin-A poses some formidable technical difficulties. The primary challenge is that vitamin-A is normally a fat-soluble molecule and any dietary intake is almost immediately sequestered away into storage within the hepatic cells of the liver. Now, with the SV40 virus randomly circulating in serum, and causing cancers throughout the body the dietary intake of regular fat-soluble vitamin-A was not going to do the trick. So, they needed to first convert the vitamin-A in to a water-soluble molecule. In doing so, it would more readily move into serum circulation, attach itself to hemoglobin, collect in the adipose tissues (the target of the soft-tissue cancers), and even into the brain. Thus, the new horrible vitamin-A palmitate molecule was made by combining retinol with palmitic acid to accomplish that goal. However, this new molecule is a perverse and unnatural molecule that almost completely circumvents the body’s natural defenses from the potential toxicity of vitamin-A. This now manmade molecule introduces more complications, and unknowns into the Project. What’s going to happen when this new water-soluble toxic molecule is introduced in to the human body? Of course, this would have been urgently tested for. However, for these biomedical Manhattan Project researchers, this was a bit like trying to squeeze a water filled balloon. As they tried to solve one problem by squeezing the balloon at the top, another one just popped out at the bottom. The new problem that popped out is the quick and catastrophic damage this new water-soluble toxic molecule does to the kidneys.
Even back in the 1930s it had been abundantly clear and proven that increased dietary levels of vitamin-A would quickly damage the kidneys, and ultimately destroy them. Here’s one such report:
Several investigators have described a pathological condition which they called hypervitaminosis A. Von Drigalski and Laubman ('33) fed six rats 1 cc. of an oil concentrate of vitamin A. These rats died in from 5 to 14 days, and post mortem examination showed glomerular nephritis with calcification to which the death of the animals was attributed.
EDWARD B. VEDDER AND CHABLES BOSENBEBG
Department of Experimental Medicine, George Washington University Medical School
(Received for publication December 17, 1937)
However, almost all the early toxicity research was done using vitamin-A as a fat-soluble molecule, typically contained in fish oils. Now, with the introduction of a new water-soluble form of vitamin-A the situation changes and gets a whole lot worse for the organ that needs to filter the body’s water-based fluids. Over most of evolutionary human history, the kidneys would have had to deal with very tiny amounts of the normally fat-soluble toxic vitamin-A molecule. But, now with vitamin-A palmitate, the toxic water-soluble form of the vitamin-A molecule is like a direct attack on the kidneys. I have little doubt that this fact was quickly discovered as they tested the vitamin-A palmitate molecule. Next, let’s move beyond the circumstantial evidence and consider some of the concrete facts.
During the time the Gottschalk Committee was at work, there were fewer than 1,000 patients being dialyzed in the entire country, but that number had increased to approximately 10,000 by the time the 1972 legislation was adopted.
http://www.nap.edu/read/1793/page/179
Okay, in 1970, there was about a grand total of fewer than 1,000 people with kidney disease in all the USA. Quite astonishingly, there are now about 660,000 people with full-blown kidney failure (needing dialysis) and about 30 million people with emerging and various other stages of kidney disease.39 That’s a gigantic 65,900% increase in just 50 years. That increase can’t be blamed on genetics, and any BS excuse of “it’s a better diagnosis” is not going to cut it either. The numbers are even more staggering when you factor in the 90,000 Americans who are killed each year by their kidney disease. Not surprisingly, today the rate of kidney disease in the USA is ten times higher than in say Russia.
Quite mysteriously, in 1972 the US government suddenly added Medicare coverage for dialysis treatment for most Americans. Why did they do that? Why did the USA adopt state funded socialized medicine for just one organ? I’ve read some vague excuses, such as “oh, it’s because dialysis treatment is really expensive”. But, so is cancer treatment, as is the care and treatment for Alzheimer’s, diabetes etc. What was so special about kidney disease that it needed this unique funding? Well, part of the reason is that 30,000,000 people is an awful lot of people.
Apparently, it looks like the real reason for the added coverage is not even part of the historical legislative record. Rather, it needs to be gleaned from legislator’s questionable recollections. Here’s a rather comprehensive report about it.
Origins of the Medicare Kidney Disease Entitlement: The Social Security Amendments of 1972
The Adoption of Section 299I
The formal legislative history of Section 299I is quite brief. The provision was not considered by the House Ways and Means Committee in hearings or in any executive session on H.R. 1. The Senate kidney amendment was added to H.R. 1 on the Senate floor, with no prior hearings, on a Saturday morning, September 30, 1972. The joint House-Senate conference committee agreed to the Senate amendment barely two weeks later. On October 30, the brief kidney provision was included in the 300-page bill signed by the President.
http://www.nap.edu/read/1793/page/179
What it looks like to me, for secretive reasons, is that they were clearly expecting a rapid increase in kidney disease, and kidney failure. Not surprisingly, this new Medicare coverage for kidney disease was hot on the heels of legislating the addition of vitamin-A palmitate into the nation’s milk supply.
You should now be asking some questions here; such as: Are you kidding me? How can there now be nearly thirty million people with kidney disease in the USA and for this to not to have been manmade? And, are you kidding me? There are now nearly thirty million people with kidney disease in the USA, and almost all of a sudden too, and almost no one is asking WHY? With all the bright minds in medical science don’t you think that by now at least someone should have asked: what’s going to happen to the kidneys when we take the highly toxic, and normally fat-soluble, vitamin-A molecule and make it water-soluble? Of course, the answer to that question was already known way back in 1950.
Conference Proceedings 1951
The authors concluded that in nephrosis (kidney disease) the power of the liver to absorb or utilize vitamin A is seriously impaired. Numerous investigations have clearly demonstrated that in conditions with impaired fat absorption vitamin A is absorbed much more efficiently from aqueous emulsions made with the Tween group of non-ionic detergents than from oily solutions.
And then again….
In chronic nephritis and urinary infections the vitamin A reserves are usually low, and often completely exhausted. Chronic nephritis is prominent among those diseases in which vitamin A is lost by urinary excretion, and in nephrosis the failure of the liver to absorb vitamin A from the blood plasma has been strongly indicated.
By T. Moore and I. M. Sharman, Dunn Nutritional Laboratory
University of Cambridge and Medical Research Council
https://doi.org/10.1079/BJN19510015
But, to the political masters overseeing the second Manhattan Project, it was like damn the torpedoes, treating millions of people with emerging kidney disease is more viable than treating millions with cancers. Clearly, they had prior knowledge that the kidney disease epidemic was about to unfold. What’s happened here is way beyond being diabolically dishonest; it is diabolically evil.
39 https://www.kidney.org/news/one-seven-american-adults-estimated-to-have-chronic-kidney-disease
An additional threat scenario needs to be considered here. Could vaccines and the supplementation of our foods with vitamin-A be some sinister and ongoing subversive military attack on the USA and other NATO countries? Probably not, but it is possible. Regardless, no terrorist organization could even dream of wreaking such massive amounts of destruction and death upon our nations.
Next, let’s review just a few of the major lies being foisted upon us by the medical establishment.
- Vitamin A is an essential nutrient.
No, it’s not, it’s a big lie. Vitamin A is the molecule that’s very likely causing most of the chronic diseases in the Western world. Additionally, the vitamin A supplementation programs are directly killing about 7,000 kids each year. - Vitamin A palmitate in sunscreens and other skin creams is safe.
No, it’s not, it’s causing the skin cancer in millions of people per year. - Food does not cause disease.
That’s a big fat lie. Of course, foods can cause disease and the wrong food is indeed the cause of most chronic disease. More specifically, it’s a poison “vitamin” causing our chronic diseases. - Food cannot cure disease.
Obviously, that too is a big fat lie. - Vaccines are safe.
The biggest and fattest lie in the world. Additionally, they’ve included an execution drug into their vaccines and have rigged the placebo testing of it. - Vaccines are effective.
No, they’re not. That’s just another big fat vaccine lie. The mumps vaccine, and others, are routinely failing to immunize and prevent the infection. - Vaccines eradicated smallpox.
No, they didn’t; not a chance of it. It’s just another big vaccine lie. - Vaccines eradicated polio.
Not very likely, and more than likely it was the polio vaccine that introduced the HIV virus into the human population. - Vaccine “science” is settled.
A blatant lie and a complete joke! Moreover, there are now 30,000,000 Americans who have mysteriously developed kidney disease, and there are 90,000 Americans (including many children) dying each year from the condition, and yet the CDC wants us to be terrorized by a mere 18 people getting the measles. The incredible irony here makes the situation completely absurd! - SIDS is the mysterious cause of death killing thousands of American infants each year.
Another big lie, because SIDS is “nothing known.” Therefore, SIDS has never killed a single infant. They know that “nothing” does not kill infants and that most of the SIDS deaths are indeed being triggered by vaccines.
Of course, the medical establishment is making an absolute killing from the frauds, lies, and peddling their fake science. Yes, regardless of trillions of our dollars being spent on the “health care crisis”, we are now the sickest, most diseased populations on the planet. We are also, by far, the sickest and most diseased populations in the history of human existence. How is that possible? It’s because we don’t have a legitimate “health care crisis”, rather we have a “disease crisis.” We have a disease crisis because we’ve been poisoned! They’ve hidden this poisoning to cover-up their colossal blunders and their complete corruption. Therefore, we must fight back and expose these frauds by doing our own real science. And, now it’s your turn to do so.
If your experiment needs statistics, you ought to have done a better experiment?
Ernest Rutherford
Hopefully, I’ve done a reasonable job of casting serious doubts on the vitamin-A deficiency theory. Of course, if the vitamin-A deficiency theory is not correct, then it leads to the next, and all important question, is vitamin-A even a vitamin at all? Regardless of what I’ve stated and all the evidence and information that I’ve presented, the answer to that question is that we still don’t know with certainty.
The great thing here is that you now get to find out for yourself. You’ll get to gather the evidence to prove it one way or the other. You’ll get to see the results firsthand. This opportunity is quite fantastic really because in many fields of science, and even more so in the medical sciences, proving or disproving a grand and long-held theory would require a lot of expertise and sophisticated equipment. That’s not the case here. Anyone can conduct this little experiment, and conclusively prove it one way or the other.
Please remember from our golden rules that if an experiment fails to support the theory, then the theory is wrong. Secondly, one person’s experimental results are not sufficient to conclusively prove the case. Others must independently repeat the experiment. Therefore, although, I’ve already conducted this experiment, and have my own results, we need your results too.
Next, remember from the early experiments that supposedly proved the vitamin-A deficiency theory, the animals quickly became very sick and died from all kinds of horrible self-destructing tissues. Very basically, the progression and sequence of events were:
- After 8 weeks, all the animals were very sick – often too weak to eat, and often developed infections
- Animals were force-fed for the remaining two-week duration
- At the 10-week mark, nearly all the animals were dead, or very close to death
- Most animals exhibited disease of the eyes and even blindness
- All animals had many internal organs and tissues disintegrating, and correspondingly had their related organ named diseases
The bottom line here, is that after 10 weeks, all animals were either extremely sick, or dead.
So, now you can conduct your own vitamin-A depletion experiments on small animals to see what really happens. However, unlike the early esteemed researchers, you are not going to use their same strange (disease inducing) diet. The key to successfully conducting this experiment is simplicity. There’s no need to overthink it or make it complicated. You don’t even need to keep notes. A simple before and after video is all that’s needed. Not only have I already conducted this experiment, I am continuing with it too. Therefore, as I outline the experimental details in the next pages, I am going to use the pronoun “we,” and not just “you.”
Basically, we are going to put two young small animals on a completely vitamin-A free diet for at least 10 weeks. When I say a vitamin-A free diet, this means not one molecule of vitamin-A, nor of any of its metabolites, nor any of its carotenoid precursors. We want no possibility of the animals getting a single molecule of vitamin-A, or any of its precursors, for the duration of the experiment. I’ll provide more diet details a bit later.
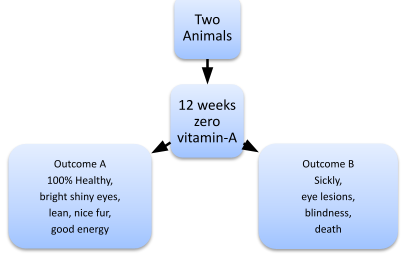
Figure 26 Outline of our experimental procedure
|
The second great thing about this experiment is we are going to make the determination of the results super simple too. The results of the experiment need to be almost binary; pass or fail.
If both the animals have all the conditions in Outcome A, then the results disprove the vitamin-A deficiency theory. However, for outcome B, if one or both the animals have even one of the conditions listed, then the results reaffirms the vitamin-A deficiency theory. In other words, it should be completely obvious what scenario the animals fall into. We don’t need a bunch of statistical analysis, or biopsies, etc. Clearly, there’s no medical degree, or Ph.D. needed here to recognize a dead rat. Seriously, even a five-year-old will be able to easily determine what category the animals fall into.
Now just to make this experiment a bit lopsided, we are going to tip the scales in favor of the Outcome-B scenario. That’s because, we are going to put the animals on a pretty restrictive diet, deplete not only in vitamin-A, but also in what many people consider other essential nutrients too. No added vitamin B, C, D or E, and no animal sourced proteins.
However, please don’t be too concerned about the animal welfare aspects of this experiment. Firstly, once again, I’ve already conducted this experiment, and the results for my animals are distinctly in the Outcome-A category. Secondly, if your animals do start to show any signs of ill health, you can immediately stop the experiment, and report your results as such.
Here’s a link to a video of my animals after ten weeks.
https://www.youtube.com/watch?v=QjpNIS9g9ZA
At eleven weeks:
https://www.youtube.com/watch?v=GxaOoFtZcU4
At thirteen weeks:
https://www.youtube.com/watch?v=pCqE2jYK8b4
|


After fourteen weeks:
https://www.youtube.com/watch?v=2MiLFsLqpuI
After eighteen weeks:
https://www.youtube.com/watch?v=itUyDGzKfTg
After twenty weeks:
https://www.youtube.com/watch?v=PhqjSlblcUs
I’ll continue to post weekly updates of them on this same YouTube channel:
https://www.youtube.com/playlist?list=PL1JNQw-cAmAGDxlBfYrfhiupYyzdlWbgh
Figure 27 is a close-up view of them at eleven weeks.
Figure 28 is a close-up photo of one of them at twenty weeks into the deplete diet.
My animals are perfectly healthy at twenty-four weeks and beyond. They have bright shiny eyes, glossy thick fur, beautiful paws, noses, tongues, ears, and tails. They are very lively, fast, yet calm and always very alert. They have never shown any sign of infection either.
Obtain two small young animals from a pet store or reputable breeder. The researchers from the 1920s-1960s mostly used small rats. Because of the jurisdiction that I live in I needed to use gerbils. You can use either pet rats, mice, or gerbils.
It is important to get young animals because we don’t want animals that have had a long time to accumulate significant amounts of vitamin-A within their liver’s. Additionally, all the early deficiency experiments clearly showed that the younger animals were more susceptible to the “deficiency” effects. Therefore, we want to reproduce these same basic experimental conditions. The animals in my experiment were about four weeks old when I bought them. That’s probably a bit borderline regarding their weaning time, but this is about the same age as many of the animals used in the original experiments of the 1920s too.
It is important to use two animals and keep them both in the same cage. Obviously, we want to get two males, or two females, not one of each gender. As you’ll learn, these are very social animals, and they need interaction and companionship. Not only are these social animals between themselves. They are surprisingly quite social with people too. In less than a week my gerbils were interactive with me too. They would come out to see me and even responded when I called them. I let them climb and scamper over my hands and develop a good sense that they were in no danger from my presence.
When I started my experiment, I had no prior experience in keeping these animals. So, there was a small learning curve to it. One thing I’d recommend is a larger cage and not one that’s too confining. I also put pieces of hard plastic pipe (for built in vacuum systems) in with their bedding. They love running through this, (unfortunately, they chew it up too). Also, these animals will kick a lot of bedding out through the side of the cage, so I put a 5-inch border around the bottom of the cage to minimize the blowout. For the bedding, I used the paper-based product and gave them about 4-inches of it. They love digging into it and making their own tunnels in it. Do not use cedar chips for bedding because it is toxic. I replace the bedding about once every 10 days.
These animals like to chew on hardwoods. I think it is somewhat essential for them to do so to prevent their teeth from growing too long. I gave my gerbils a block of maple hardwood to chew on. Of course, they need a good water supply. I just used the standard small animal water bottle. I cleaned their food dish every day. Obviously, we don’t want to place their cage in direct sunlight, or under a bright lamp. That’s about it for the housekeeping details, now on to the details of the diet.
Like with the other aspects of this experiment, we can keep the diet super simple too. There are just three hard rules in this experiment. These rules can never, ever, be violated. Not even once.
- No vitamin-A, or precursor – not from any possible source
- No foods from animal sources
- Nothing that will directly harm them
To make sure that the animals get no vitamin-A, we need to rule out all possible sources completely. Unlike the bizarre sickening diets used by the earlier researchers, we are not going to give them any source of animal fats. Therefore, of course, not one speck of butter, or lard, or milk, or any milk products. Just to be extra safe, there’s not to be one molecule of food from animal sources, and therefore no animal based protein, and no egg products. The only foods allowed are from plant sources, and only plant sources that are documented to have zero molecules of vitamin-A and zero molecules of the carotenoids.
I just need to be extra clear here. Any plant-based foods labeled as having 0% RDA of vitamin-A does not mean they have zero molecules of vitamin-A or its precursors. Flax seed is not allowed either since it is a source of the lutein and zeaxanthin carotenoids. Therefore, regardless of what any label claims, no fruits, no vegetables, no lettuce, no grass, and not even straw is allowed. Once again, we want them to have absolutely no possible source of vitamin-A.
For the third rule, we also don’t want to give them any foods that can harm them, such as candies, chocolate, refined sugars, citrus, other manmade vitamins, etc. Also, I don’t let my gerbils chew on household cardboard because I am not sure of what glues and other compounds it might contain.
Unlike the earlier deficiency researchers, we are going to let the animals decide for themselves what they are going to eat. We are not going to ration their food, and we are not going to measure and record how much they eat. It does not matter how much they eat, just give them as much as they want. Also, unlike the earlier researchers, we are not going to mix their food into proportioned pellets, and we are not going to force them to eat salt. No, the animals get to pick and choose for themselves what foods they will eat each day, albeit from a very limited a la carte menu. Of course, under no circumstances should any food ever be forced on the animals.
Here’s the list of foods that I fed my gerbils, in no particular order.
- Partially-cooked rolled oats40 – they seemed to like this food the most
- Cooked brown rice – their second most favorite food
- Puffed brown rice (with no additives whatsoever)
- Cooked black beans (with no sauces)
- Roasted macadamia nuts – they somewhat liked these
- Hempseed – not sure if they ate much of it
- Peanuts – they did not like peanuts, not sure if they ate much of it if any
My animals showed little interest in white rice, so I did not provide it too often. Very occasionally, I gave them a few lightly salted potato chips (ingredients potatoes and sunflower seed oil). Although I did not provide it, cauliflower would be a great addition to this diet.
40 Basically, this is uncooked oatmeal. Oatmeal in Canada is not supplemented with VA. Do not use “steel cut” oats, as it is often not cooked at all.
Let’s go. It can’t get simpler than that. Just do it! Record a video of the animals on day one, and another on day 85 and beyond. Then share your results.
When I first bought my gerbils (two males) they were a bit plump, but not too much so. Also, since they were only four weeks old at the time, they had some growing to do. On this diet, they most certainly did grow bigger. But, as they grew bigger they also grew leaner. They remained completely healthy, with bright shiny eyes, and always maintained very nice fur. They also always appeared vibrant, and quite playful. So, I was not too concerned about the lean bodies. After all, what guy wants to be “plump” looking anyway?
When I was at the pet store buying my young gerbils, there was one gerbil in the candidate group who appeared to be having a seizure; it was like an epileptic seizure. The sales person told me not to worry and assured me that seeing seizures in gerbils was quite normal. Well, that may be so when on their pet store diet. But, what I want to assure you of, is that no, seizures are not normal. I have never seen my gerbils exhibit any seizure or anything even remotely close to it. On the contrary, my animals appear calm and show amazing agility and balance. However, if your animals do start having seizures, I suggest that there’s something seriously wrong, and you end the experiment, and of course, report your results too.
A few people have suggested to me that having now proven that my gerbils remained completely healthy for more than 12 weeks on a zero vitamin-A diet, that I should now go the other direction on it. They have suggested that I dose them up on vitamin-A to see what happens.
Well, I’ve already conducted this little add-on experiment on a human, yes myself. The results were quick, brutally painful, infecting, and just downright extremely nasty. So, no, I have no desire to inflict this torture on my little gerbils. I rather like my gerbils, and I don’t want to harm them. Moreover, I have no need to do the vitamin-A toxicity experiment, because it has already been conducted at least a thousand times over, on lab animals. I have no doubt whatsoever as to what the results will be. Therefore, no, I am not going to dose up my gerbils on vitamin-A. What you do with your animals, post-experiment, say past the 24-week timeframe, is up to you.

Figure 29 Gerbils at 24 weeks without “wet tail”
Our tails tell no tales. You see, we’re all good down there. |
Additionally, when I bought my gerbils, the sales person insisted that I buy an antibiotic solution that was supposed to be added to their daily water. They told me without it; the gerbils would eventually develop diarrhea and a condition called “wet tail.” To appear to be a well-intentioned new pet owner, I bought it. However, I’ve never used it, not one drop of it. My gerbils have not ever exhibited a need for it. They have never developed diarrhea or “wet tail.”
Seriously, why would we expect these animals to develop “wet tails” without manmade antibiotics? These animals in nature are not going to the pharmacy to dose up on antibiotics. Even more ironically, the antibiotic solution would probably slowly destroy their natural gut flora, and then that would then cause them to develop chronic diarrhea.
Nothing, absolutely nothing. They remain perfectly healthy. Therefore, I think it’s rather clear that so-called vitamin-A is not a vitamin. Not at all. It is most likely only what we know it to be; and that is that it is a toxin.
Now, it’s up to you. If you think I am right about this, then you must repeat this experiment. If you think I am wrong about this, then you must repeat this experiment. Either way, you must repeat this experiment and publish your results. Please understand that participation in this is not optional. It is now a requirement of being a citizen. You are not allowed just to sit there and do nothing. You are not allowed to leave this up to someone else. Every day we delay more kids will slip into autism, more infants will mysteriously die from SIDS, more young women will be diagnosed with breast cancer, more men will be diagnosed with pancreatic or prostate cancer, more teenagers are going to be diagnosed with untreatable IBD and have their colon cut out. Many other teenagers are going to be diagnosed with ADHD, or chronic depression etc. And these new diagnoses are all going to continue nonstop and it’s going to be repeated day, after day, after day.
Of course, that’s just scratching the surface of the situation. Like with the body being composed of billions of cells, as more of those cells become sick and damaged then the overall body gets sick, and eventually dies too. The same applies to our society. Consider each person as being an important cell the makes up our societal body. As more and more people get sick and diseased the overall stress and pressure on our society spreads and grows with it. We, as an overall society become sick, and it will eventually destroy our nations. There is simply no way, we, as a society can survive the exponential rates of chronic diseases we are currently witnessing. Once again, I am not trying to sound dramatic, or alarmist; that’s just a fact.
If our small animal experiment is repeated and verified by many other people, and hopefully by many people from around the world too, then this will obviously confirm that the vitamin A deficiency experiments from the 1920s were indeed botched. That confirmation will also then, of course, invalidate the evidence used to first define vitamin A as being a vitamin. With that understanding, we can then cross vitamin-A off the list of the official vitamins.
However, our animal experiment does not conclusively prove that some storage levels of the retinol molecule might not have some very long-term, and yet unknown beneficial effect. Who knows, maybe the body has a novel need for a toxic molecule that mimics poison ivy?
Therefore, my current plan is to continue with the experiment and keep my gerbils on a zero vitamin-A diet for the remainder of their lives. Although this diet is devoid of many other nutrients, and not just that of vitamin-A, I want to see what the very long-term consequences of zero vitamin-A intake are. My guess is that my animals are going to live way past the normal one to two-year life expectancy for this species. After all, with no artificial driver promoting the “differentiation” of their stem cells, their stem cell populations will be maintained much longer. If an extended lifespan proves to be true, then I think it will be safe to conclude that vitamin-A is not necessary for sustaining animal life, at all. Once again, this would need to be verified thousands of times over too.
But, let’s not be distracted too much here with debunking just the vitamin-A theory. Our real overarching goal is in determining if the overload of vitamin-A is the root cause of the autoimmune diseases, and many of the psychiatric disorders too. That determination is going to require many more experiments (by human volunteers who are currently suffering from these diseases going on very low, and ideally zero, vitamin A diets) to conclusively prove it one way or the other. Except now, no one should have any fear of going blind while conducting this experiment.
As with my animal experiment, I too plan on remaining on a near zero retinol and beta-carotene diet for the rest of my life. My personal diet is documented in my previous e-book, but I’m re-summarizing it here for convenient reference. The only modification that I’ve made to that diet in the last year is that I’ve removed the flax seed (not that I was including it very often anyways), and the pineapple.
I want to emphasize that I am not using the term diet here in the traditional sense of the word. This diet is not at all about weight loss or even nutrition. I also do not want to give any connotation that this is a good diet. This diet is simply a collection of foods with ample nutrition, and that doesn’t contain a chemical that is now a direct toxin to myself.
- Lots of water
- White or brown rice (not yellow or golden!)
- Beef (steak, roast, ideally cooked in a slow cooker, no sauces, or spices other than salt and trace amounts of pepper if wanted). Bison would be even better than beef.
- Cauliflower
- Black pinto beans*
- Olive oil (max of 1 teaspoon per day)
- Black coffee if wanted (no milk no cream, no whiteners)
- Zinc, Vitamin C, and B supplements if wanted
* For a while I did include red kidney beans in my diet. I’ve since dropped them due to their carotenoid content.
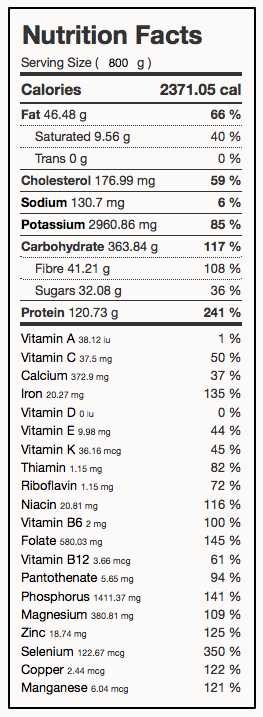 |
However, this diet is most certainly not skimpy on nutrition or calories either. Based on the proportions shown below, here’s the approximate nutrition label41 for this daily diet.
| Food | Amount(g) |
| Rice (white/brown) | 240 |
| Roast Beef | 175 |
| Kidney / Pinto Beans | 100 |
| Olive oil | 10 |
| Honey | 20 |
| Pineapple | 50 |
I very occasionally included some applesauce, pineapple, and a few almonds. These can help with fiber, provide vitamin C, E and make an otherwise dry rice and beef meal quite delicious too. However, it is critically important not to overdo it on the olive oil or almonds. Both are quite high in vitamin E, and this too can become toxic at too high a level. Vitamin E is also documented to cause an increase in serum vitamin A levels too. This elevated risk is because the body is now reaching its capacity for storing any of the fat-soluble vitamins in general. Additionally, depending on if you routinely include some pineapple and or apple sauce or not, you’ll probably want to supplement with vitamin C. Vitamin C is critically important ammunition needed by the immune system to fight off cancer development, and pathogens. If you get bored of the red meat, you can substitute turkey breast, and you might even splurge on lobster every now and then. Therefore, this is most certainly not a starvation diet either. To try to go even lower on inadvertent retinol consumption, I’ve replaced my beef consumption with bison. I’ve also cut back quite a bit on my olive oil consumption and have completely cut out avocado oil due to its lutein content.
Thank you.
41 Nutrition label produced with nutrient.bio.
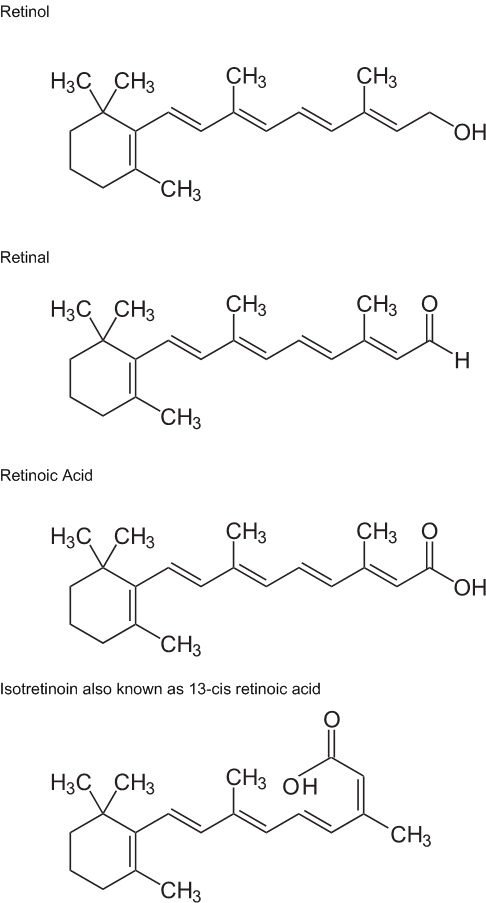
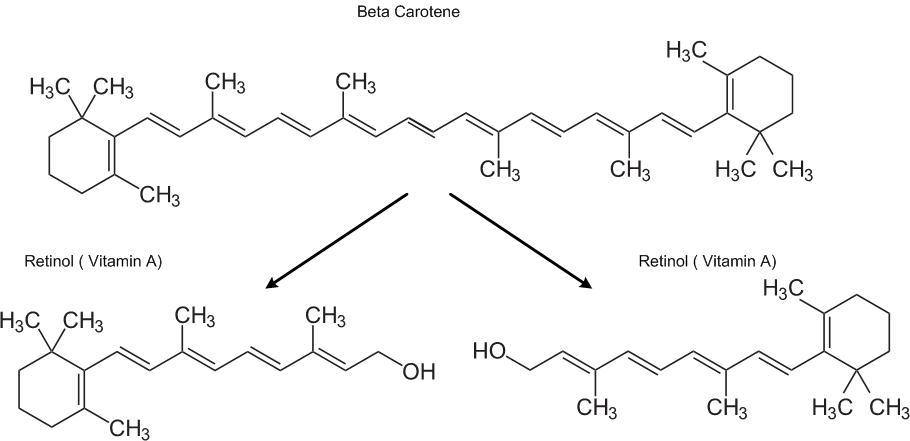
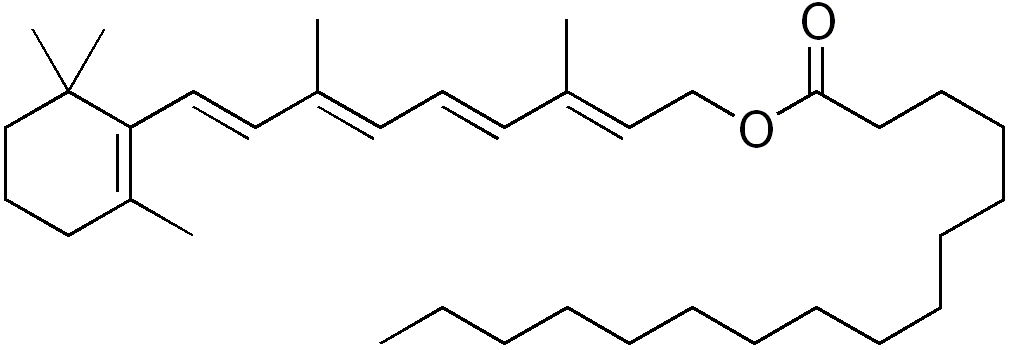

| Figure 1 The trapdoor Retinol consumption cycle Figure 2 Killer-cell activity stimulated into action with retinoic acid Figure 3 The basal keratinocytes driven onto the wrong path Figure 4 The stratified epithelial of the skin Figure 5 The skin cell’s interlocking tight junctions Figure 6 The shed off outer layers of the epidermis – resulting in “mush” Figure 7 The destroyed epidermis – leading to infections Figure 8 Liberated men from the Japanese P.O.W. camps Figure 9 Faces and eyes of emaciated men at the Dachau Figure 10 Young emaciated men liberated from the Dachau camp Figure 11 The eyes of a starved Russian man from the Dachau Camp Figure 12 Relative mortality rates with vitamin-A supplementation Figure 13 Photodecomposition and Phototoxicity of Natural Retinoids Figure 14 Alzheimer’s death rate age group 55-65 Figure 15 Alzheimer’s death rate age group 65-75 Figure 16 Alzheimer’s death rate age group 75-85 Figure 17 Autoimmune Disease Incidence Rates Figure 18 Children with Autism served by IDEA Figure 19 Some chronic disease incidence rate disparities per 100,000 Figure 20 SIDS deaths in relation to date of recent DTP vaccination Figure 21 Immune cells investigating vaccine caused inflammation Figure 22 Immune cells finding a food protein included in the vaccine Figure 23 Worldwide Melanoma of Skin Cancer Incidence - 2008 Figure 24 Doctors killing with Syringes: Phenol Injections Figure 24 Snippet of the CDC infant vaccine schedule Figure 26 Our simple experimental process Figure 27 Gerbils at eleven weeks on the VA free diet Figure 28 Gerbil close-up view at twenty weeks on the VA free diet Figure 29 Gerbils at 24 weeks without “wet tail” |
12 14 20 20 20 23 23 50 50 50 50 56 66 71 71 71 71 71 72 81 93 93 98 99 100 105 105 105 115 |
| Table 1 Classification of Xerophthalmia conditions Table 2 Mean concentration of triglycerides in males and females Table 3 Attributes of human vision Table 4 Example disease incidence rate disparities by country Table 5 The Top Food Allergies in the USA |
4 32 66 71 93 |